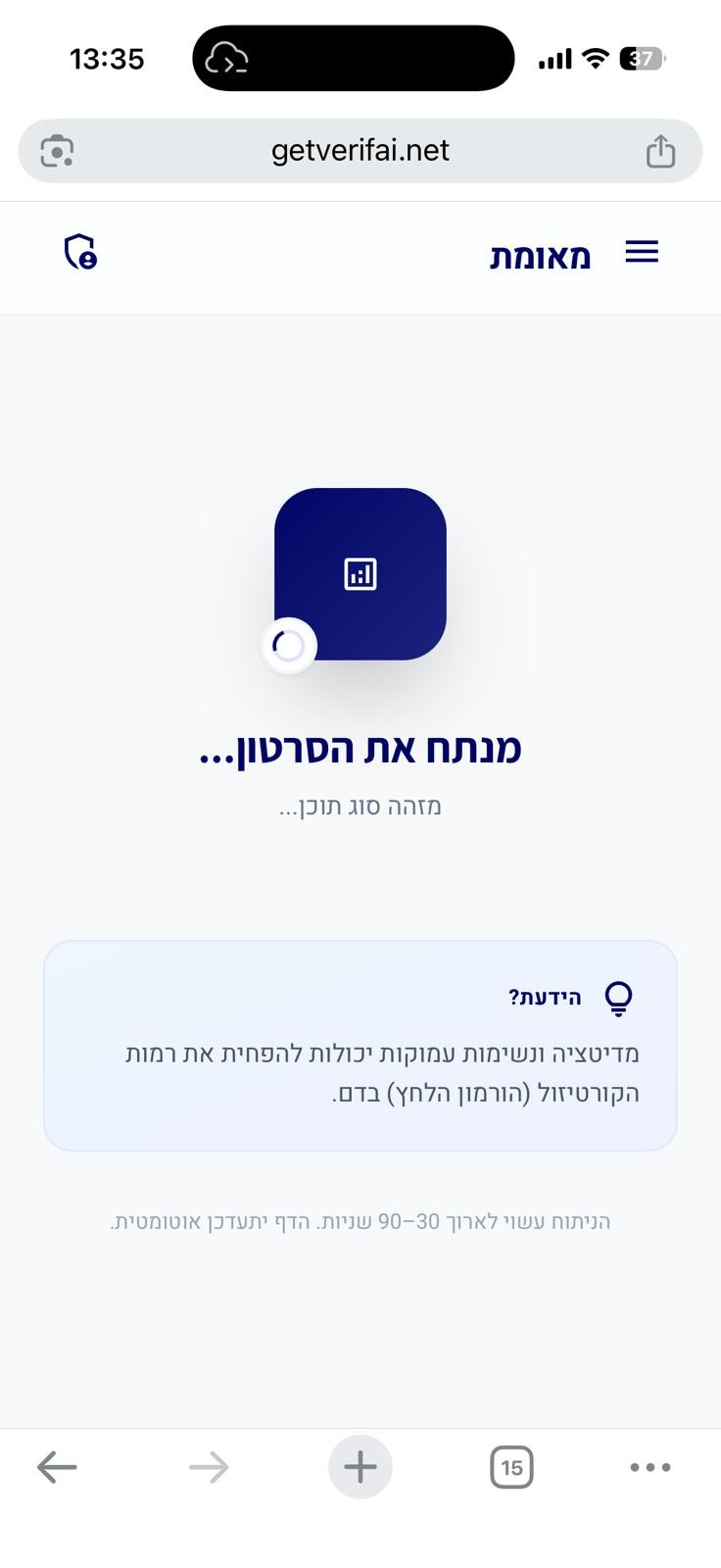
סריקה בתהליך...
הניתוח עשוי לארוך 30–90 שניות
הידעת?
הסרטון אינו מכיל תוכן רפואי
חושבים שחלה טעות?
אם לדעתכם הסרטון אכן עוסק בטענות רפואיות או בריאותיות, הוסיפו הסבר קצר ושלחו בקשה לבדיקה מחדש.
הבקשה התקבלה! נבדוק את הסרטון ונחזור אליכם.
אירעה שגיאה בשליחת הבקשה. נסו שוב.
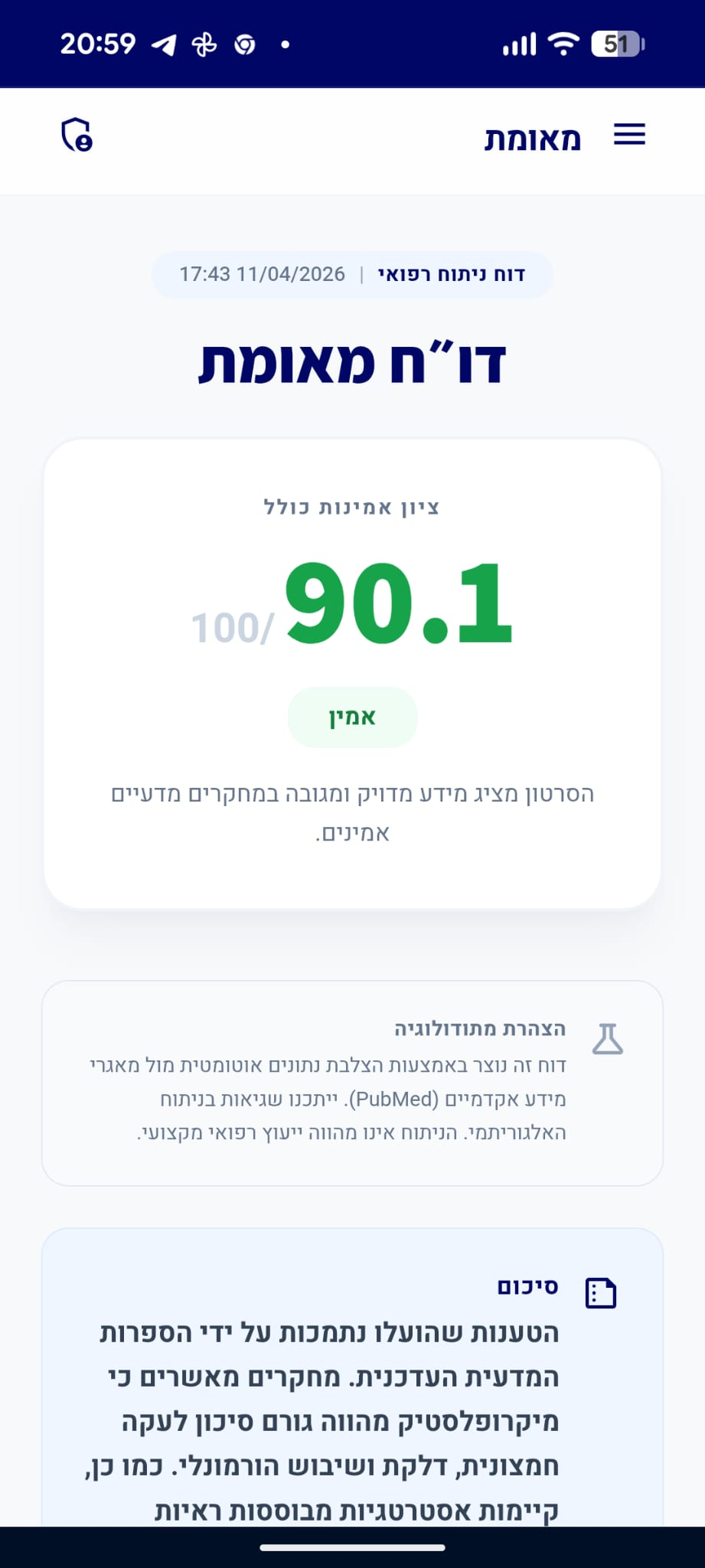
דו״ח מאומת
הסרטון מציג מידע מדויק ומגובה במחקרים מדעיים אמינים.
סיכום
הטענות שהוצגו בנוגע לפתופיזיולוגיה של צרבת, הביטויים החוץ-וושטיים שלה, חשיבות הירידה במשקל והתועלת בטיפול תרופתי למניעת סיבוכים נתמכות היטב על ידי הספרות המדעית ב-PubMed. הטענה לגבי לעיסת מסטיק אינה מגובה במאמרים שסופקו בהקשר זה, אך שאר הטענות נמצאו מדויקות ומבוססות ראיות.
analytics ניתוח טענות מבוסס ראיות
"לעיסת מסטיק ללא סוכר אחרי האוכל מעלה את ייצור הרוק, שעוזר לנטרל ולשטוף חומצה שעלתה לוושט."
מסקנת הבדיקה:
לא סופקו מאמרים מדעיים בטקסט המצורף המאששים את הטענה לגבי לעיסת מסטיק, ולכן לא ניתן לאמת אותה על סמך המקורות שניתנו, למרות שהיא מהווה המלצה נפוצה בפרקטיקה הקלינית. (⬜)
"סימפטומים של צרבת נגרמים עקב מעבר של חומצה, מלחי מרה ואנזימים מהקיבה לעבר הוושט."
מסקנת הבדיקה:
הספרות המדעית מאשרת כי מחלת החזר קיבתי-וושטי (GERD) נגרמת כתוצאה מחדירת תוכן קיבה, הכולל חומצה, מלחי מרה ואנזימים, אל הוושט, מה שמוביל לתסמינים ולנזק לרקמות. (🟩)
chevron_right מקורות מדעיים: (3)
-
link
Pathophysiology of Gastroesophageal Reflux Disease.
The pathogenesis of gastroesophageal reflux disease (GERD) is complex and involves changes in reflux exposure, epithelial resistance, and visceral sensitivity. The gastric refluxate is a noxious material that injures the esophagus and elicits symptoms. Esophageal exposure to gastric refluxate is the primary determinant of disease severity. This exposure arises via compromise of the anti-reflux barrier and reduced ability of the esophagus to clear and buffer the refluxate, leading to reflux disease. However, complications and symptoms also occur in the context of normal reflux burden, when there is either poor epithelial resistance or increased visceral sensitivity. Reflux therefore develops via alterations in the balance of aggressive and defensive forces.…
PMID: 29037470
-
link
GERD pathogenesis, pathophysiology, and clinical manifestations.
Gastroesophageal reflux disease (GERD) is a specific clinical entity defined by the occurrence of gastroesophageal reflux through the lower esophageal sphincter (LES) into the esophagus or oropharynx to cause symptoms, injury to esophageal tissue, or both. The pathophysiology of GERD is complex and not completely understood. An abnormal LES pressure and increased reflux during transient LES relaxations are believed to be key etiologic factors. Prolonged exposure of the esophagus to acid is another. Heartburn and acid regurgitation are the most common symptoms of GERD, although pathologic reflux can result in a wide variety of clinical presentations. GERD is typically chronic, and while it is generally nonprogressive, some cases are associated with development of complications of increasing severity and significance.…
PMID: 14705378
-
link
Pathophysiology of Gastroesophageal Reflux Disease.
<p>Background: Gastroesophageal reflux disease (GERD) is a prevalent gastrointestinal disorder caused by the retrograde flow of gastric contents into the esophagus, leading to bothersome symptoms and complications. Its pathophysiology is complex and multifactorial, and recent research has aimed to explain the heterogeneity of GERD phenotypes, each influenced by different underlying mechanisms that contribute to symptom presentation and disease progression. Summary: GERD arises from an imbalance between defensive mechanisms and disruptive factors. Key pathophysiological contributors include esophageal gastric junction dysfunction, transient lower esophageal sphincter relaxations, esophageal motility abnormalities, delayed gastric emptying, and thoracoabdominal pressure gradients. Mucosal damage is exacerbated by prolonged exposure to acid and bile, pepsin activity, and impaired esophageal volume and chemical clearance. Additionally, central and peripheral neural modulation influences symptom perception, with heightened visceral sensitivity and esophageal hypervigilance playing significant roles in symptom severity and treatment response. Emerging diagnostic techniques such as high-resolution manometry, impedance-pH monitoring, and EndoFLIP® are improving our ability to identify specific pathophysiological abnormalities, leading to more personalized approaches to GERD management. Key Messages: (i) GERD results from a multifactorial interplay between anatomical, functional, and neurophysiological mechanisms. (ii) Esophageal clearance, EGJ structure and function, acid exposure, mucosal resistance, and neural modulation are crucial determinants of symptom severity and disease progression. (iii) The presence of different phenotypes of the reflux disease (e.g., GERD, functional heartburn, and reflux hypersensitivity) underscores the need for individualized diagnostic and therapeutic strategies. (iv) Advances in diagnostic technologies enhance our understanding of GERD pathophysiology, facilitating tailored management approaches beyond acid suppression therapies. Future research should focus on refining GERD phenotyping and integrating mechanistic insights into personalized treatment paradigms. </p>.…
PMID: 40562014
"צרבת/ריפלוקס יכולה להיות קשורה גם לשיעול כרוני, טעם מר בפה, ריח רע מהפה, דלקת גרון, טריגר לאסתמה ואפילו שחיקת שיניים."
מסקנת הבדיקה:
מחקרים קליניים מכירים בביטויים חוץ-וושטיים של ריפלוקס, הכוללים שיעול כרוני, דלקת גרון, אסתמה ושחיקת שיניים, כתוצאה מחשיפת דרכי הנשימה והפה לתוכן הקיבה. (🟩)
chevron_right מקורות מדעיים: (3)
-
link
Extraesophageal manifestations in gastroesophageal reflux disease.
Gastroesophageal reflux disease (GERD) is a common condition that affects about 20-30% of the adult population, presenting with a broad spectrum of symptoms and varying degrees of severity and frequency. Other manifestations are being increasingly recognized: the so-called ''extraesophageal'' manifestations, such as laryngitis, hoarseness, chronic cough, asthma, or non-cardiac chest pain. Epidemiological studies consistently demonstrate significant associations between pulmonary manifestations and GERD. Up to 50% of patients with an endoscopically proven esophagitis suffer from symptoms other than heartburn or acid regurgitation. However, the published estimates of extraesophageal disorders in patients with GERD vary widely, which may be a result of referral bias. The most effective initial approach in suspected reflux-related extraesophageal symptoms is empiric proton pump inhibitor (PPI) therapy. However, studies demonstrated that the advantage of long-term PPI treatment over placebo could have been overestimated.…
PMID: 16971871
-
link
Extraesophageal manifestations of gastroesophageal reflux disease: real or imagined?
Extraesophageal reflux disease is a common clinical presentation to gastroenterology as well as ear, nose and throat, allergy, and asthma clinics. The diagnosis and management of this condition is challenging. We review the current dilemma in this area and discuss the latest studies which help guide our therapies for patients with suspected extraesophageal reflux. Diagnostic approach to patients with extraesophageal reflux disease involved the use of insensitive tools, which have hampered the ability to correctly identify patients at risk. Empiric trial using proton pump inhibitors is still the recommended initial approach to those suspected of having reflux as the cause for extraesophageal symptoms such as asthma, chronic cough, or laryngitis. Diagnostic testing should be reserved to those unresponsive to therapy. Most recent studies suggest that ambulatory impedance/pH monitoring performed on therapy may be most likely to help exclude reflux as the cause for persistent symptoms. Recent randomized placebo-controlled studies on chronic laryngitis, cough, and asthma have been disappointing in showing benefit of acid suppressive therapy. Gastroduodenal reflux may cause symptoms such as chronic cough, asthma, or laryngitis. However, we are currently limited in our diagnostic ability to identify the subgroup of patients who might respond to acid suppressive therapy. Impedance/pH monitoring may be a step in the right direction; however, outcome studies are needed to better understand the role of acid or nonacid reflux in patients with extraesophageal symptoms.…
PMID: 20473157
-
link
Diagnostic and Management Approach to Reflux-Related Cough.
Chronic cough, defined as cough persisting longer than 8 weeks, affects approximately 10% of the global population and significantly impairs quality of life. Gastroesophageal reflux disease is a recognized cause of chronic cough, yet the relationship remains complex and poorly understood. Up to 75% of patients with reflux-related cough lack classic gastroesophageal symptoms such as heartburn or regurgitation, making diagnosis particularly challenging. Although direct tissue irritation by refluxate has been proposed as a primary mechanism, evidence also supports a vagally mediated esophageal- tracheobronchial reflex. Cough hypersensitivity is also recognized as an important mechanism, amplifying responses to reflux and contributing to persistent symptoms despite reflux-directed therapy. Diagnostic evaluation requires a structured approach integrating clinical assessment, empiric treatment trials, and objective testing including ambulatory reflux monitoring. Upper endoscopy may reveal reflux complications, but most patients with reflux-related cough have normal endoscopic findings. Management involves a stepwise approach beginning with lifestyle modifications and proton pump inhibitor therapy, with neuromodulators and behavioral interventions reserved for refractory cases. Surgical intervention may benefit carefully selected patients but requires shared decision-making regarding risks and benefits. Development of more accurate diagnostic tools and unified clinical guidelines will be critical for advancing the management of this difficult-to-treat condition. This article reviews reflux-related cough, including its diagnostic evaluation and management strategies.…
PMID: 41646078
"ירידה במשקל של אפילו מספר ק"ג יכולה לעזור להפחית את הלחץ התוך-בטני ולהקל על צרבת, וזהו הגורם המשמעותי ביותר שניתן לשלוט בו."
מסקנת הבדיקה:
הספרות המדעית מצביעה על קשר ישיר בין השמנה, לחץ תוך-בטני מוגבר וצרבת. ירידה במשקל מוכרת כאסטרטגיה טיפולית משמעותית להפחתת הלחץ על הסוגר הוושטי התחתון. (🟩)
chevron_right מקורות מדעיים: (3)
-
link
Gastro-oesophageal reflux disease in obesity: pathophysiological and therapeutic considerations.
Gastro-oesophageal reflux disease (GERD) is common in obese patients. Apart from the physical discomfort and the economic burden, GERD may increase morbidity and mortality through its association with oesophageal carcinoma. The pathophysiology of GERD differs between obese and lean subjects. First, obese subjects are more sensitive to the presence of acid in the oesophagus. Second, hiatal hernia, capable of promoting GERD by several mechanisms, is more prevalent among the obese. Third, obese subjects have increased intra-abdominal pressure that displaces the lower oesophageal sphincter and increases the gastro-oesophageal gradient. Finally, vagal abnormalities associated with obesity may cause a higher output of bile and pancreatic enzymes, which makes the refluxate more toxic to the oesophageal mucosa. The altered body composition associated with obesity affects the pharmacokinetics of drugs. There are no data regarding the efficacy of any of the drugs used for GERD treatment. The dosages of cimetidine and ranitidine should be calculated according to the patient's ideal body weight, not their actual weight. Of the operative procedures used for weight loss, Roux-en-Y gastric bypass was found to be most effective for GERD, while gastric banding was associated with a high prevalence of reflux. This review outlines the pathophysiology and the treatment of GERD in obesity with emphasis on the therapeutic considerations in this population of patients.…
PMID: 12119661
-
link
Single-stage transoral incisionless fundoplication and laparoscopic sleeve gastrectomy for the management of GERD and obesity.
Gastro-esophageal reflux disease (GERD) is frequently associated with obesity. Excess body weight, particularly central adiposity, with a concomitantly raised intra-abdominal pressure, leads to a reduced lower esophageal sphincter (LES) pressure and GERD. The lax LES essentially causes acid reflux in the lower esophagus. We report a 44-year-old woman who presented to our surgical clinic with heartburn and acid reflux, associated with difficulty in weight management. The patient had a BMI of 35 kg/m The patient was planned for a single-stage Transoral Incisionless Fundoplication (TIF) and laparoscopic sleeve gastrectomy for her GERD and obesity, respectively. TIF was performed by two experienced endoscopists, one controlling the EsophyX device and the other ensuring continuous direct visualization of the field of work with the endoscope. Following the procedure, laparoscopic sleeve gastrectomy was performed during the same session. The patient had an uneventful recovery. Eight months after surgery, the patient reported resolution of her GERD symptoms and a weight loss of 20 kg.…
PMID: 36996706
-
link
Patients with Obesity Undergoing Roux-En-Y Gastric Bypass Versus Fundoplication for Refractory GERD: A Systematic Review and Meta-Analysis.
Gastroesophageal reflux disease (GERD) significantly impairs quality of life and is associated with complications such as Barrett’s esophagus and esophageal adenocarcinoma. Obesity exacerbates GERD pathophysiology by elevating intra-abdominal pressure, making treatment more difficult. Current evidence suggests that Roux-en-Y gastric bypass (RYGB) offers superior outcomes compared to fundoplication in patients with severe obesity (BMI ≥ 40 kg/m²). This review aims to critically evaluate fundoplication versus RYGB in the population with obesity and GERD. We conducted a systematic review and meta-analysis in accordance with PRISMA guidelines. We performed a comprehensive search across PubMed, Embase, and Cochrane databases for studies comparing fundoplication versus RYGB in patients with obesity and GERD. Data extraction was standardized, focusing on intraoperative complications, operative time, length of hospital stay, reoperation, postoperative complications, postoperative dysphagia, and DeMeester score. Statistical analysis was performed using Cochrane RevMan (Review Manager 9.7.1), employing random-effects models. Heterogeneity was assessed using Cochran’s Q test and I² statistic. The analysis included 7 observational studies. We found no differences in complication rates after sensitivity analysis. There were no differences in dysphagia, reoperation rate, operative time and length of stay. At a weighted mean follow-up of 42.3 months (range: 19.6 to 52.0) for fundoplication and 35.2 months (range: 14.6 to 49.0) for RYGB, GERD resolution, measured by the DeMeester score, slightly favored fundoplication, although the absolute difference was not clinically relevant. Regarding weight outcomes, RYGB demonstrated significantly higher total weight loss (TWL) at the 12-month follow-up. Fundoplication appears statistically superior for GERD resolution postoperatively, but the difference is not clinically relevant. RYGB has a higher TWL. Both procedures are safe for GERD control in patients with obesity. The choice between procedures should weigh reflux severity, complication risks, and metabolic diseases associated with obesity. Larger studies are needed to clarify the impact of surgical timing and patient-specific factors. The online version contains supplementary material available at 10.1007/s11695-026-08552-1.…
PMID: 41838365
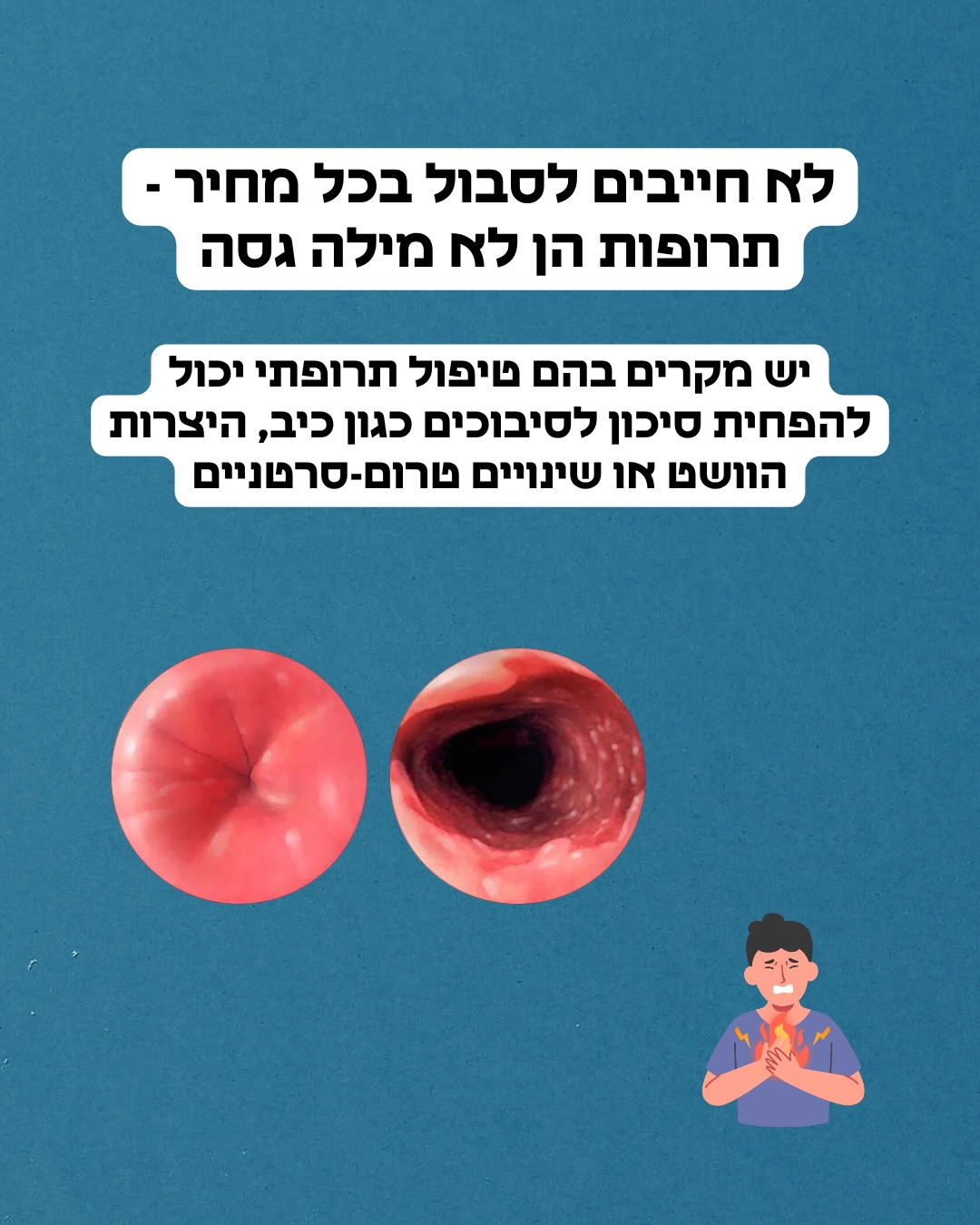
"יש מקרים בהם טיפול תרופתי יכול להפחית סיכון לסיבוכים כגון כיב, היצרות הוושט או שינויים טרום-סרטניים."
מסקנת הבדיקה:
טיפול תרופתי בצרבת נועד להפחית את החשיפה לחומצה, ובכך למנוע סיבוכים ארוכי טווח כגון כיבים, היצרויות בוושט ושינויים טרום-סרטניים כמו ושט על שם בארט. (🟩)
chevron_right מקורות מדעיים: (2)
-
link
Gastroesophageal Reflux Disease.
Gastroesophageal reflux disease (GERD) is a condition that occurs when reflux of gastric contents into the esophagus causes symptoms and/or complications. The prevalence of GERD in Western societies has been estimated at 30%, making it one of the most commonly encountered disorders in primary care. The spectrum of GERD includes typical symptoms of esophageal reflux (heartburn and/or regurgitation); esophageal injury (erosive esophagitis; stricture; Barrett esophagus; and, rarely, adenocarcinoma); and extraesophageal symptoms, such as hoarseness and chronic cough. Proper diagnosis and treatment of GERD includes symptom control, exclusion of other disorders, avoiding overuse of medications and invasive testing, and minimizing complications.…
PMID: 39133924
-
link
Barrett's esophagus.
Gastroesophageal reflux disease (GERD) is a condition commonly managed in the primary care setting. Patients with GERD may develop reflux esophagitis as the esophagus repeatedly is exposed to acidic gastric contents. Over time, untreated reflux esophagitis may lead to chronic complications such as esophageal stricture or the development of Barrett's esophagus. Barrett's esophagus is a premalignant metaplastic process that typically involves the distal esophagus. Its presence is suspected by endoscopic evaluation of the esophagus, but the diagnosis is confirmed by histologic analysis of endoscopically biopsied tissue. Risk factors for Barrett's esophagus include GERD, white or Hispanic race, male sex, advancing age, smoking, and obesity. Although Barrett's esophagus rarely progresses to adenocarcinoma, optimal management is a matter of debate. Current treatment guidelines include relieving GERD symptoms with medical or surgical measures (similar to the treatment of GERD that is not associated with Barrett's esophagus) and surveillance endoscopy. Guidelines for surveillance endoscopy have been published; however, no studies have verified that any specific treatment or management strategy has decreased the rate of mortality from adenocarcinoma.…
PMID: 15152957

ד״ר אסי שגיב
דירוג זה מבוסס על 1 דוחות אימות קודמים.






האם הדוח הזה היה מועיל לך?
מה היה פחות טוב? (רשות)
תודה על הפידבק!
עירעור על דוח זה
ספקו ראיות חדשות או הצביעו על אי דיוקים
נעדכן אותך על תוצאות הבדיקה
הוסיפו קישורים למחקרים או מקורות רפואיים מוכרים
העירעור נשלח בהצלחה!
המנוע המדעי שלנו יבדוק את הראיות שהגשתם. נעדכן אתכם באימייל עם התוצאות.
ניתוח מבוסס בינה מלאכותית
דוח זה נוצר באופן אוטומטי על ידי מערכת בינה מלאכותית ועשוי להכיל שגיאות, אי-דיוקים או מידע חלקי. הניתוח אינו מהווה ייעוץ רפואי, אבחנה או המלצה לטיפול, והוא אינו תחליף לדעתו של איש מקצוע רפואי מוסמך. יש להתייעץ עם רופא או מומחה מוסמך לפני קבלת כל החלטה רפואית. המידע מוצג לצרכי מידע כללי בלבד.
מידע זה מופק על ידי בינה מלאכותית ואינו מהווה תחליף לייעוץ רפואי מקצועי.