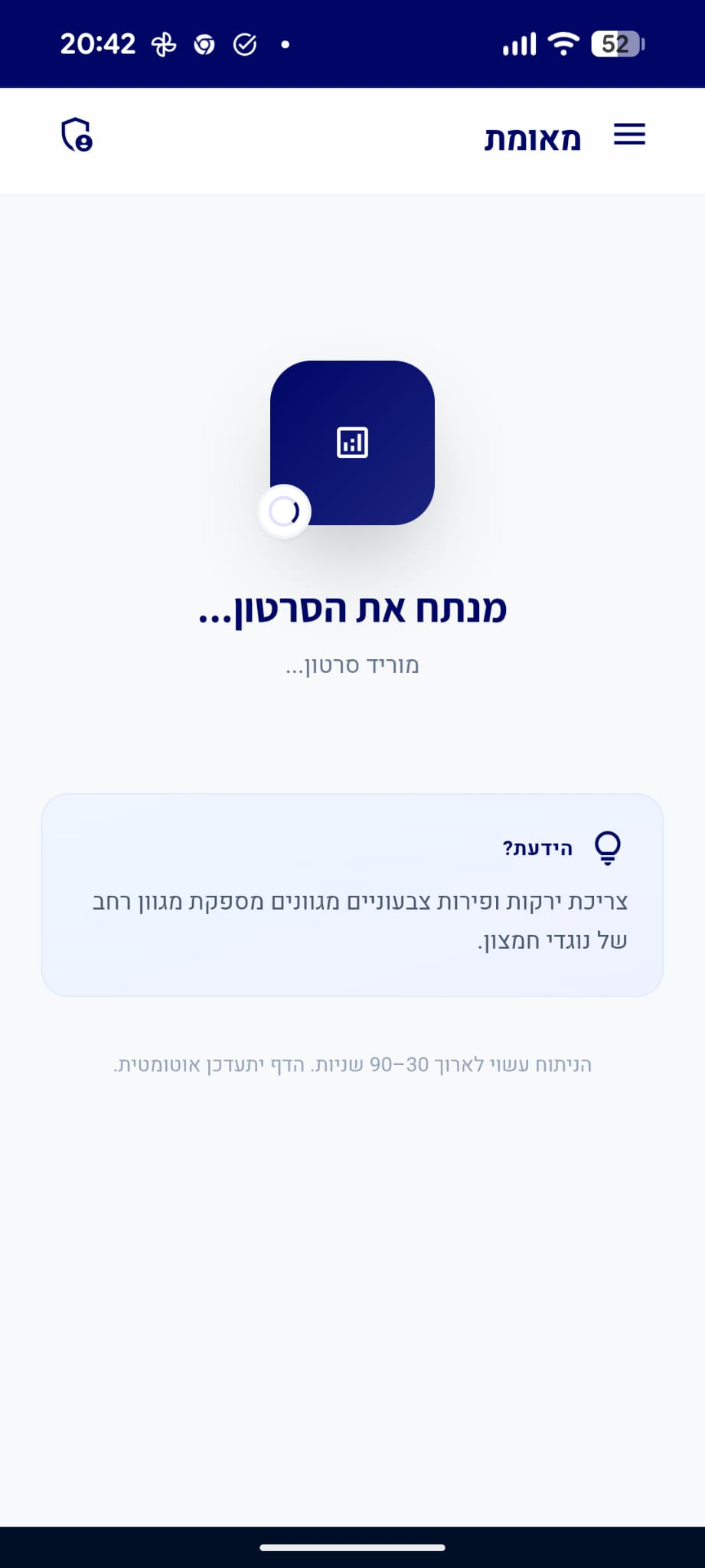
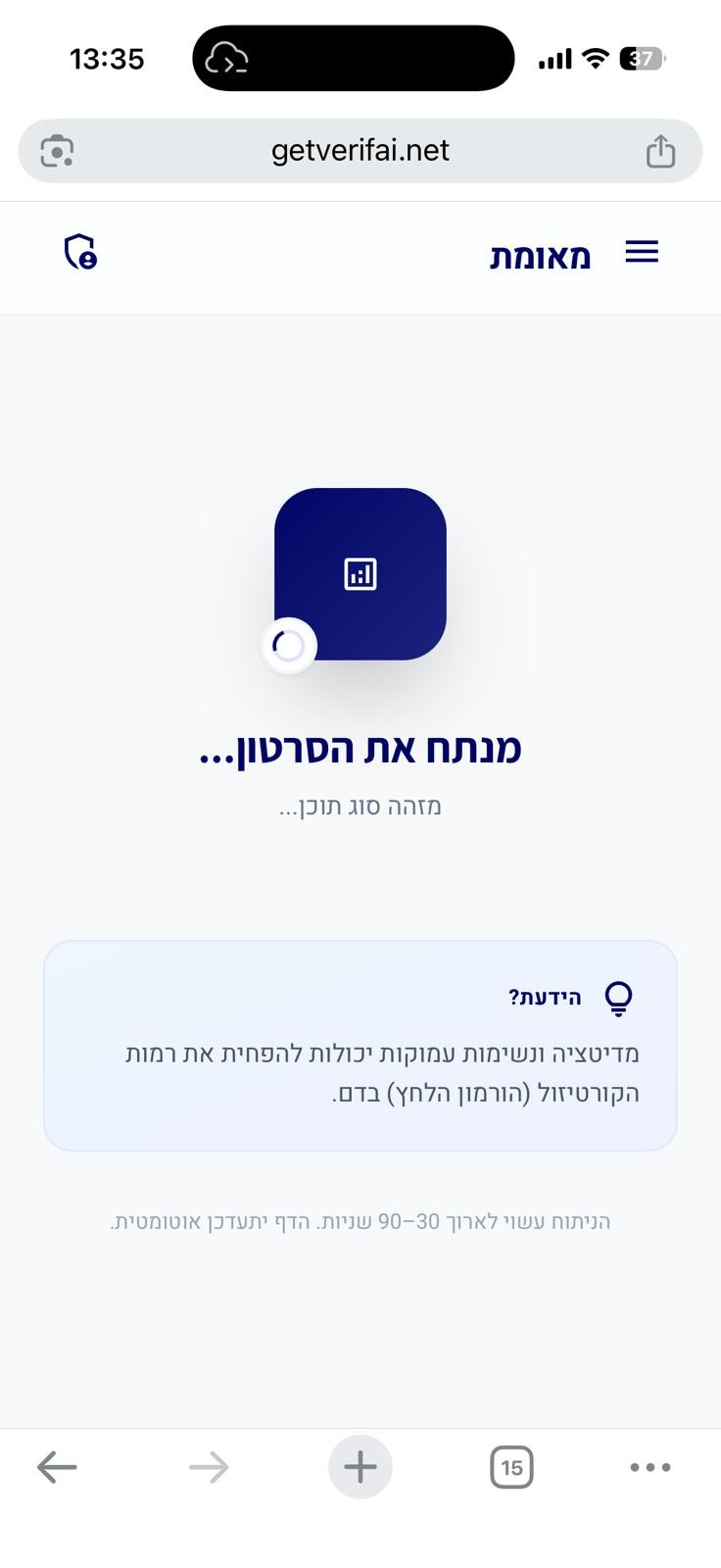
סריקה בתהליך...
הניתוח עשוי לארוך 30–90 שניות
הידעת?
הסרטון אינו מכיל תוכן רפואי
חושבים שחלה טעות?
אם לדעתכם הסרטון אכן עוסק בטענות רפואיות או בריאותיות, הוסיפו הסבר קצר ושלחו בקשה לבדיקה מחדש.
הבקשה התקבלה! נבדוק את הסרטון ונחזור אליכם.
אירעה שגיאה בשליחת הבקשה. נסו שוב.
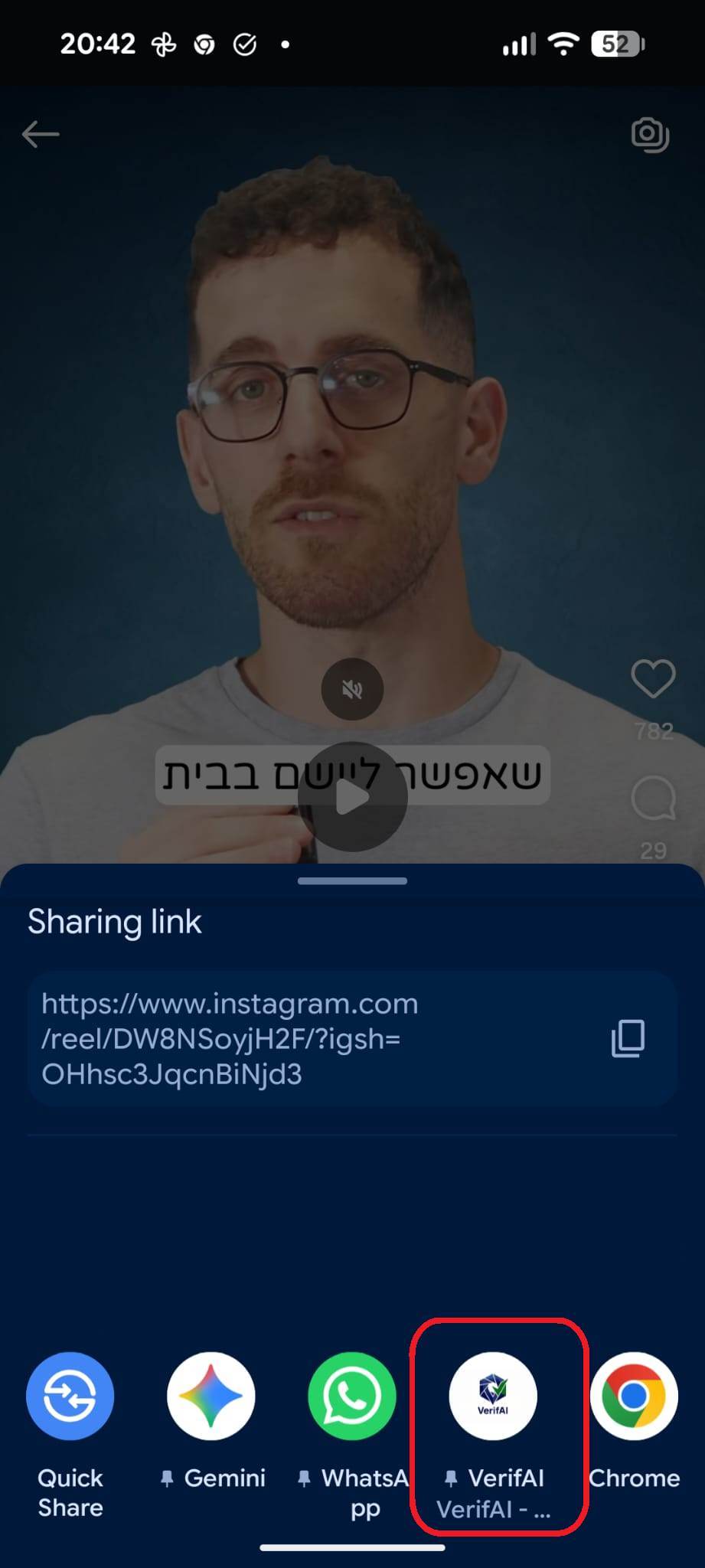
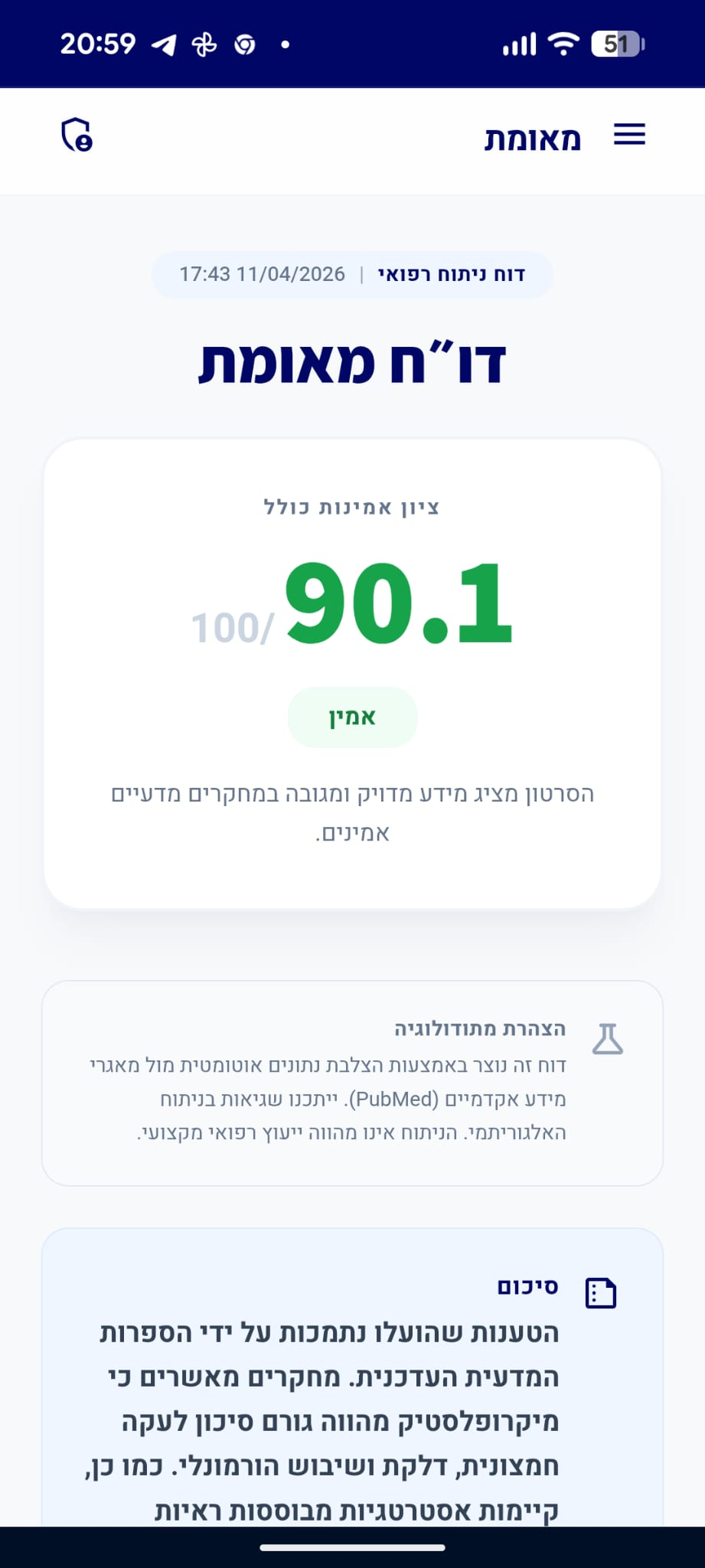
דו״ח מאומת
הסרטון מציג מידע מדויק ומגובה במחקרים מדעיים אמינים.
סיכום
הסרטון מציג מידע רפואי מדויק התואם את הקונצנזוס המדעי. הטענות לגבי התנדפות אלכוהול והשפעתו על העובר מאומתות, וההמלצה להימנע מאלכוהול בהיריון לחלוטין היא הסטנדרט הרפואי המקובל, שכן לא הוגדרה רמת חשיפה בטוחה.
analytics ניתוח טענות מבוסס ראיות
"צריכה חד-פעמית של כמות קטנה מאוד של אלכוהול כרוכה בסיכון נמוך מאוד."
מסקנת הבדיקה:
בעוד שהסיכון המוחלט מחשיפה חד-פעמית קטנה עשוי להיות נמוך סטטיסטית, הקהילה הרפואית נמנעת מלהגדיר זאת כ'בטוח' ומדגישה כי אין סף ידוע לחשיפה ללא סיכון, ולכן ההמלצה הגורפת נותרת הימנעות מוחלטת. (🟨)
chevron_right מקורות מדעיים: (2)
-
link
Alcohol use: less is better. An umbrella systematic review of clinical interventions, policies, and dose-response health risks in adults.
<h4>Background</h4>Alcohol is a major modifiable cause of morbidity, premature mortality and health inequalities, yet evidence informing "low-risk" thresholds and prevention strategies is fragmented.<h4>Methods</h4>Umbrella systematic review conducted according to PRISMA 2020 (protocol on OSF). PubMed/MEDLINE and Scopus were searched (Jan 2015-Mar 2026). An overlap-management approach selected an anchor synthesis per research question (Q1-Q37); supporting records were retained for triangulation. Quality appraisal used design-appropriate tools. Synthesis was narrative.<h4>Results</h4>Of 14,991 records, 49 were included (46 systematic reviews/meta-analyses, 2 WHO documents, 1 cross-sectional study) covering 37 pre-specified questions. Across most outcomes, higher intake and riskier patterns were associated with higher risk, with harms evident at levels often labelled 'moderate'. Any drinking increased injury odds (OR 2.80). Dose-response evidence showed steep gradients for cirrhosis (RR 9.35 in women and 2.82 in men at 40 g/day) and small but measurable increases in selected cancers at light drinking (e.g., breast cancer RR 1.05). In primary care, brief interventions reduced consumption at 12 months by -20 g/week. Pricing measures and some availability restrictions were directionally associated with lower consumption and harms, whereas evidence for other policy levers was more heterogeneous.<h4>Conclusions</h4>Overall evidence favoured lower alcohol intake and avoidance of heavy episodic drinking, although confidence varied by endpoint and was limited for several questions by the quality of the available syntheses. Apparent low-dose benefits were not robust to bias-aware analyses. These findings support a pragmatic counselling and policy message of "less is better" rather than a universal safe threshold.…
PMID: 41887989
-
link
The effect of moderate gestational alcohol consumption during pregnancy on speech and language outcomes in children: a systematic review.
Consensus has not been reached on safe alcohol consumption recommendations during pregnancy. The National Institutes for Care and Health Excellence (NICE) in the UK suggest that one to two drinks not more than twice per week is safe. However, the speech and language effects of even low levels of alcohol use among offspring are unknown. The aim of this study was to review systematically the evidence on studies of the effect of low to moderate levels of alcohol consumption during pregnancy (up to 70 grams of alcohol per week) compared to abstinence on speech and language outcomes in children. Using medical subject headings, PubMed, Web of knowledge, Scopus, Embase, Cinahl and the Cochrane Library were searched from their inception up to March 2012. Case control and cohort studies were included. Two assessors independently reviewed titles, abstracts and full articles, extracted data and assessed quality. A total of 1,397 titles and abstracts were reviewed of which 51 full texts were retrieved. Three cohort studies totaling 10,642 women met the inclusion criteria. All three studies, (United States (2) and Australia (1)) indicated that language was not impaired as a result of low to moderate alcohol consumption during pregnancy. Two studies were judged to be of low quality based on a six-item bias classification tool. Due to heterogeneity, results could not be meta-analyzed. Studies included in this review do not provide sufficient evidence to confirm or refute an association between low to moderate alcohol use during pregnancy and speech and language outcomes in children. High quality, population based studies are required to establish the safety of low to moderate levels of alcohol use such as those set out by the NICE guidelines in the UK.…
PMID: 24383422
"בתהליך האפייה או הבישול, מולקולות אתנול מתנדפות בגלל טמפרטורת רתיחה נמוכה של 78 מעלות צלזיוס."
מסקנת הבדיקה:
אתנול אכן בעל נקודת רתיחה של כ-78 מעלות צלזיוס, מה שגורם להתנדפותו בתהליכי חימום, אם כי קצב ההתנדפות תלוי במשתנים רבים כמו זמן הבישול, הטמפרטורה ושטח הפנים. (🟩)
"חלק מהאלכוהול נשאר במזון גם לאחר סיום תהליך האפייה או הבישול."
מסקנת הבדיקה:
מחקרים מראים כי תהליכי בישול ואפייה אינם מבטיחים סילוק מוחלט של אלכוהול, ושאריות אתנול נותרות במזון בהתאם לשיטת ההכנה והזמן. (🟩)
"אין כמות אלכוהול שנחשבת בטוחה לצריכה במהלך הריון בכל שלב שהוא."
מסקנת הבדיקה:
ארגוני בריאות מובילים בעולם קובעים כי לא הוגדרה כמות בטוחה לצריכת אלכוהול במהלך ההיריון, בשל הסיכון להתפתחות הפרעות על רצף האלכוהול העוברי (FASD). (🟩)
chevron_right מקורות מדעיים: (2)
-
link
Italian Guidelines for the diagnosis and treatment of Fetal Alcohol Spectrum Disorders.
Drinking alcohol during pregnancy can cause congenital disabilities. J. Roquette, P. Lemoine and K.L. Jones were the first to describe these effects. In 1973, Jones and Smith coined the term Fetal Alcohol Syndrome to describe children with facial anomalies, poor growth, and learning difficulties. The caution against drinking during pregnancy has existed for centuries, including in The Bible (Judges 13:3-4). Maternal alcohol consumption is linked to congenital disabilities. To ensure safety, it is advised to abstain from alcohol during pregnancy. Fetal Alcohol Spectrum Disorder (FASD) was observed in paintings from the mid-19th century when artists began depicting moments and characters from everyday life. In 2005-2006, Italy conducted a groundbreaking study on FASD, the first in Europe. The study resulted in valuable research on FASD, contributing to prevention efforts. Unfortunately, diagnosing FASD remains a challenge in Italy. Early diagnosis and treatment are critical, and increasing the number of authorized centers to diagnose FASD is necessary to improve care. Educating ourselves about FASD is the key to creating a world where affected children receive the care they need. These guidelines include nine works dealing with all FASD aspects such as prevention, the effects on cognition, the epidemiology, the diagnostic criteria, the clinical aspects, the general effects on the body, the available treatments and the methods of detecting alcohol abuse in pregnant women.…
PMID: 39470670
-
link
Alcohol use and pregnancy consensus clinical guidelines.
to establish national standards of care for the screening and recording of alcohol use and counselling on alcohol use of women of child-bearing age and pregnant women based on the most up-to-date evidence. published literature was retrieved through searches of PubMed, CINAHL, and the Cochrane Library in May 2009 using appropriate controlled vocabulary (e.g., pregnancy complications, alcohol drinking, prenatal care) and key words (e.g., pregnancy, alcohol consumption, risk reduction). Results were restricted to literature published in the last five years with the following research designs: systematic reviews, randomized control trials/controlled clinical trials, and observational studies. There were no language restrictions. Searches were updated on a regular basis and incorporated in the guideline to May 2010. Grey (unpublished) literature was identified through searching the websites of health technology assessment (HTA) and HTA-related agencies, national and international medical specialty societies, clinical practice guideline collections, and clinical trial registries. Each article was screened for relevance and the full text acquired if determined to be relevant. The evidence obtained was reviewed and evaluated by the members of the Expert Workgroup established by the Society of Obstetricians and Gynaecologists of Canada. The quality of evidence was evaluated and recommendations were made according to guidelines developed by the Canadian Task Force on Preventive Health Care. the quality of evidence was rated using the criteria described by the Canadian Task Force on Preventive Health Care (Table 1). the Public Health Agency of Canada and the Society of Obstetricians and Gynaecologists of Canada. these consensus guidelines have been endorsed by the Association of Obstetricians and Gynecologists of Quebec; the Canadian Association of Midwives; the Canadian Association of Perinatal, Women's Health and Neonatal Nurses (CAPWHN); the College of Family Physicians of Canada; the Federation of Medical Women of Canada; the Society of Rural Physicians of Canada; and Motherisk. SUMMARY STATEMENTS: 1. There is evidence that alcohol consumption in pregnancy can cause fetal harm. (II-2) There is insufficient evidence regarding fetal safety or harm at low levels of alcohol consumption in pregnancy. (III) 2. There is insufficient evidence to define any threshold for low-level drinking in pregnancy. (III) 3. Abstinence is the prudent choice for a woman who is or might become pregnant. (III) 4. Intensive culture-, gender-, and family-appropriate interventions need to be available and accessible for women with problematic drinking and/or alcohol dependence. (II-2). 1. Universal screening for alcohol consumption should be done periodically for all pregnant women and women of child-bearing age. Ideally, at-risk drinking could be identified before pregnancy, allowing for change. (II-2B) 2. Health care providers should create a safe environment for women to report alcohol consumption. (III-A) 3. The public should be informed that alcohol screening and support for women at risk is part of routine women's health care. (III-A) 4. Health care providers should be aware of the risk factors associated with alcohol use in women of reproductive age. (III-B) 5. Brief interventions are effective and should be provided by health care providers for women with at-risk drinking. (II-2B) 6. If a woman continues to use alcohol during pregnancy, harm reduction/treatment strategies should be encouraged. (II-2B) 7. Pregnant women should be given priority access to withdrawal management and treatment. (III-A) 8. Health care providers should advise women that low-level consumption of alcohol in early pregnancy is not an indication for termination of pregnancy. (II-2A).…
PMID: 21172102
"אלכוהול עובר דרך השלייה לעובר, אשר אינו מסוגל לפרק אותו ביעילות כמו מבוגר."
מסקנת הבדיקה:
אלכוהול עובר את השלייה בקלות ומגיע לעובר, אשר מערכות האנזימים שלו אינן בשלות מספיק כדי לפרק את האלכוהול ביעילות, מה שמוביל לחשיפה ממושכת ופגיעה התפתחותית. (🟩)

Jordan Ovadia | ירדן עובדיה
דירוג זה מבוסס על 9 דוחות אימות קודמים.

האם הדוח הזה היה מועיל לך?
מה היה פחות טוב? (רשות)
תודה על הפידבק!
עירעור על דוח זה
ספקו ראיות חדשות או הצביעו על אי דיוקים
נעדכן אותך על תוצאות הבדיקה
הוסיפו קישורים למחקרים או מקורות רפואיים מוכרים
העירעור נשלח בהצלחה!
המנוע המדעי שלנו יבדוק את הראיות שהגשתם. נעדכן אתכם באימייל עם התוצאות.
ניתוח מבוסס בינה מלאכותית
דוח זה נוצר באופן אוטומטי על ידי מערכת בינה מלאכותית ועשוי להכיל שגיאות, אי-דיוקים או מידע חלקי. הניתוח אינו מהווה ייעוץ רפואי, אבחנה או המלצה לטיפול, והוא אינו תחליף לדעתו של איש מקצוע רפואי מוסמך. יש להתייעץ עם רופא או מומחה מוסמך לפני קבלת כל החלטה רפואית. המידע מוצג לצרכי מידע כללי בלבד.
מידע זה מופק על ידי בינה מלאכותית ואינו מהווה תחליף לייעוץ רפואי מקצועי.