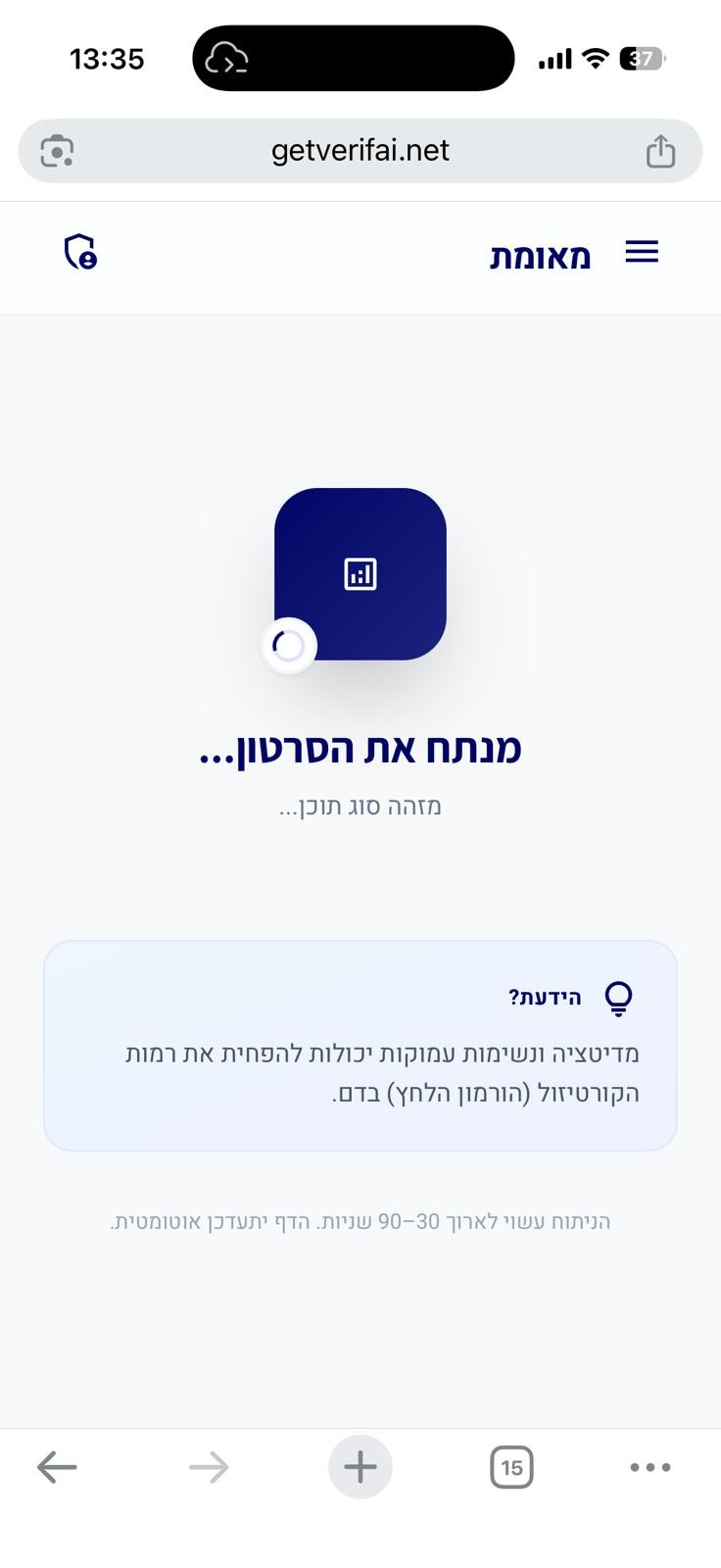
סריקה בתהליך...
הניתוח עשוי לארוך 30–90 שניות
הידעת?
הסרטון אינו מכיל תוכן רפואי
חושבים שחלה טעות?
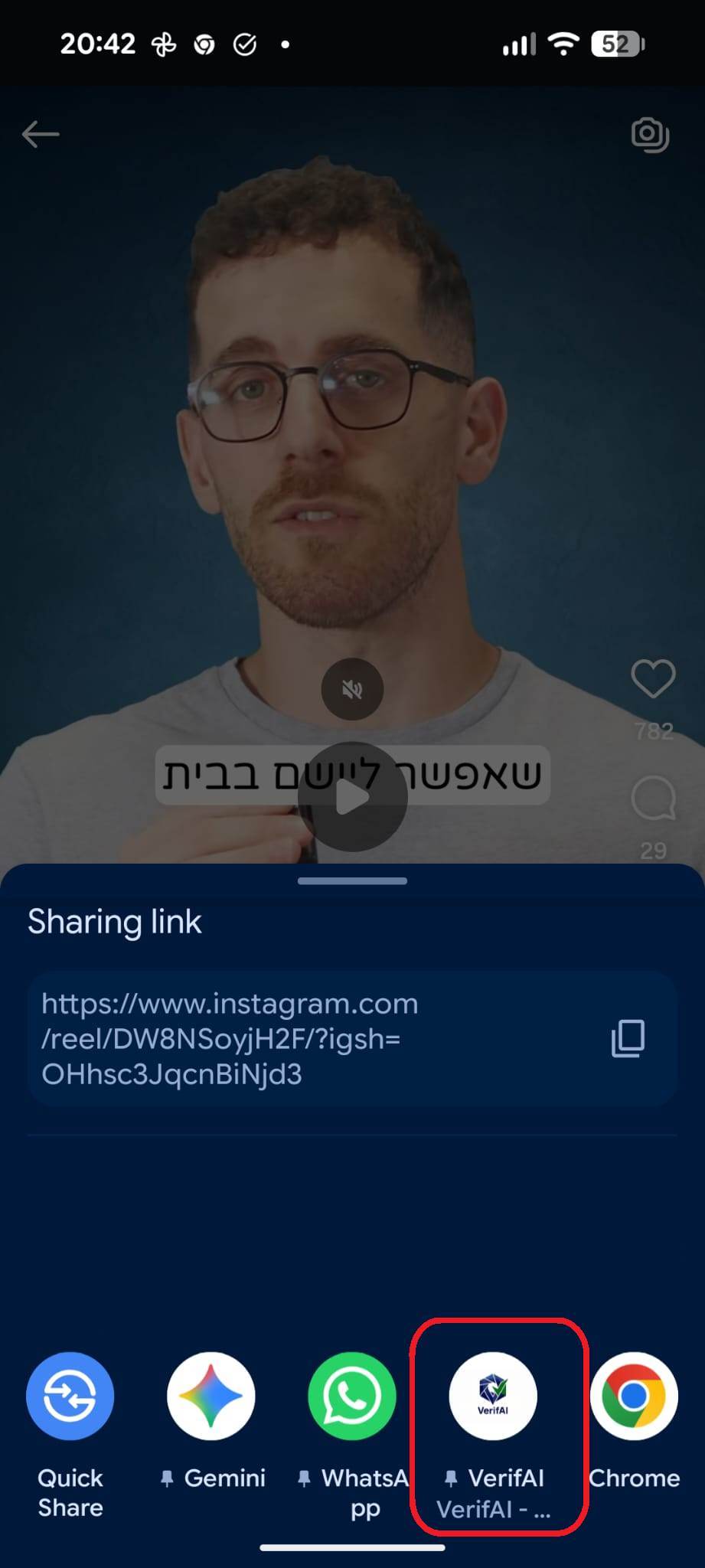
אם לדעתכם הסרטון אכן עוסק בטענות רפואיות או בריאותיות, הוסיפו הסבר קצר ושלחו בקשה לבדיקה מחדש.
הבקשה התקבלה! נבדוק את הסרטון ונחזור אליכם.
אירעה שגיאה בשליחת הבקשה. נסו שוב.
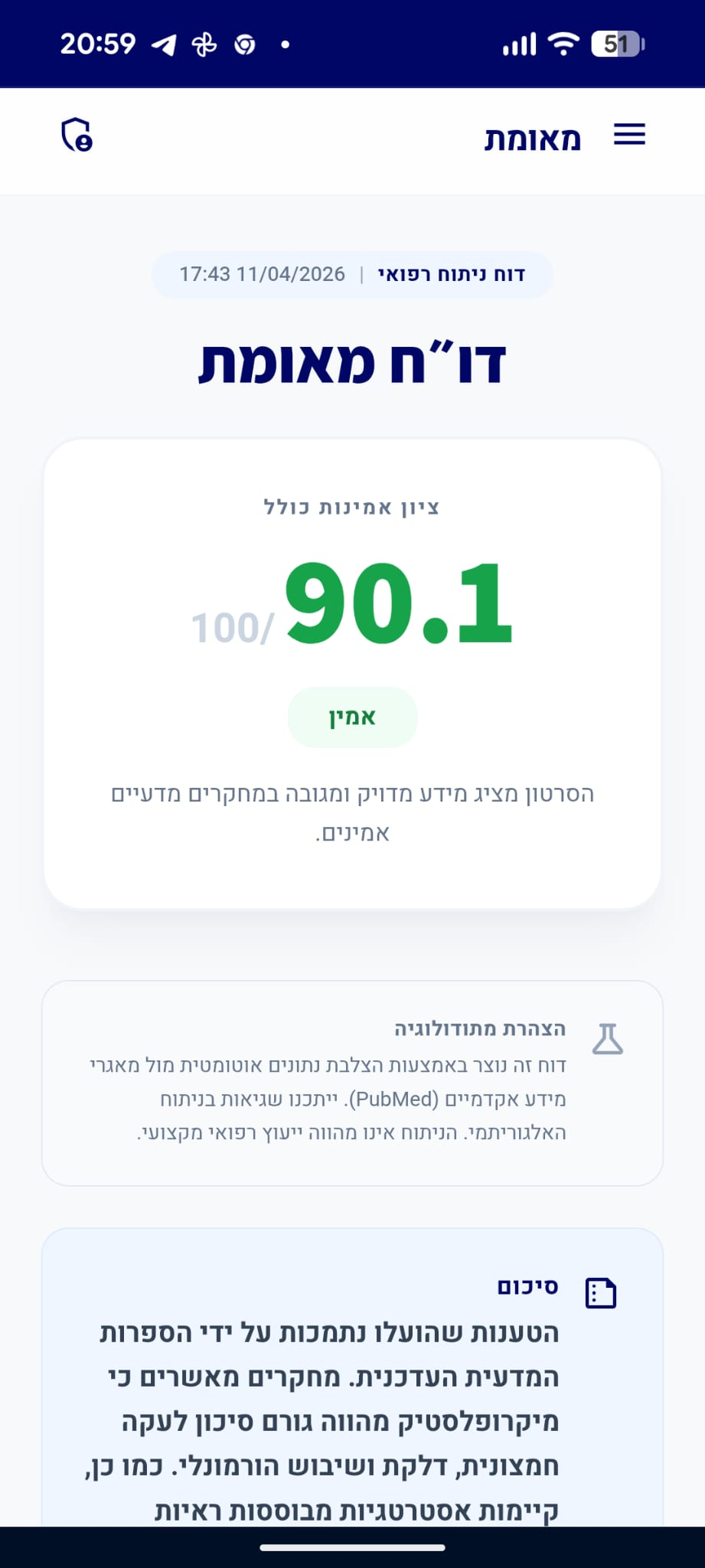
דו״ח מאומת
הסרטון מכיל שילוב של עובדות מוכחות וטענות המטעות את הציבור.
סיכום
הקליפים הציגו הליכה של 18,000 ו-40,000 צעדים ביום כהישג גופני, בעוד המומחה טען כי הליכה מוגזמת (מעל 15,000 צעדים) עלולה להזיק למפרקים, במיוחד בהיעדר מסת שריר מספקת. בעוד שהספרות המדעית מאשרת את חשיבות מסת השריר להגנה על המפרקים, לא נמצאו ראיות התומכות בטענה כי הליכה בטווחים אלו גורמת לנזק מפרקי, וההמלצות המדעיות על מספר צעדים אופטימלי אינן כוללות סף נזק כפי שצוין. לכן, הטענות לגבי נזק מהליכה מרובה נותרות ללא ביסוס מחקרי מוצק.
דוח על סרטון תגובה
סרטון זה מציג קליפ של אדם המביע טענות רפואיות, ומומחה/מגיב שמתייחס אליהן. הציון מבוסס רק על טענות המומחה.
quiz טענות הקליפ ותגובת המומחה
"10,000 צעדים ביום."
"הליכה של 15,000 עד 25,000 צעדים ביום עלולה לפגוע במפרקים."
המומחה מזהיר מפני הליכה מוגזמת שמוצגת בקליפים כהישג.
מסקנת הבדיקה:
לא נמצאה עדות מדעית חד-משמעית ב-PubMed התומכת בכך שהליכה בטווח של 15,000-25,000 צעדים גורמת כשלעצמה לנזק למפרקים באוכלוסייה בריאה. הספרות המדעית מדגישה לרוב את היתרונות של פעילות גופנית, גם עבור אנשים עם שחיקת מפרקים. (⬜)
"18,000 צעדים ביום."
info המומחה לא התייחס ישירות לטענה זו ואין מספיק נתונים לבדיקה עצמאית
"40,000 צעדים ביום."
info המומחה לא התייחס ישירות לטענה זו ואין מספיק נתונים לבדיקה עצמאית
person_check טענות נוספות של המומחה
טענות שהמומחה הביע שאינן קשורות ישירות לטענה ספציפית בקליפ
"הטווח המומלץ לצעדים ביום הוא: 2,800 (מינימום), 7,000 (אידיאלי), 8,000 (שיפור מטבולי), 10,000 (תועלת קלה), ומעל 15,000 (עלול לגרום לנזק)."
מסקנת הבדיקה:
בעוד שמחקרים מצביעים על ירידה בסיכון לתמותה החל מ-2,500-3,000 צעדים ביום, אין הסכמה מדעית על טווחים ספציפיים כ'אידיאליים' או על קביעה כי מעל 15,000 צעדים גורמים לנזק. הנתונים מראים לרוב קשר של תועלת עולה עם עלייה במספר הצעדים. (🟨)
chevron_right מקורות מדעיים: (2)
-
link
Relationship of Daily Step Counts to All-Cause Mortality and Cardiovascular Events.
The minimal and optimal daily step counts for health improvements remain unclear. A meta-analysis was performed to quantify dose-response associations of objectively measured step count metrics in the general population. Electronic databases were searched from inception to October 2022. Primary outcomes included all-cause mortality and incident cardiovascular disease (CVD). Study results were analyzed using generalized least squares and random-effects models. In total, 111,309 individuals from 12 studies were included. Significant risk reductions were observed at 2,517 steps/d for all-cause mortality (adjusted HR [aHR]: 0.92; 95% CI: 0.84-0.999) and 2,735 steps/d for incident CVD (aHR: 0.89; 95% CI: 0.79-0.999) compared with 2,000 steps/d (reference). Additional steps resulted in nonlinear risk reductions of all-cause mortality and incident CVD with an optimal dose at 8,763 (aHR: 0.40; 95% CI: 0.38-0.43) and 7,126 steps/d (aHR: 0.49; 95% CI: 0.45-0.55), respectively. Increments from a low to an intermediate or a high cadence were independently associated with risk reductions of all-cause mortality. Sex did not influence the dose-response associations, but after stratification for assessment device and wear location, pronounced risk reductions were observed for hip-worn accelerometers compared with pedometers and wrist-worn accelerometers. As few as about 2,600 and about 2,800 steps/d yield significant mortality and CVD benefits, with progressive risk reductions up to about 8,800 and about 7,200 steps/d, respectively. Additional mortality benefits were found at a moderate to high vs a low step cadence. These findings can extend contemporary physical activity prescriptions given the easy-to-understand concept of step count. (Dose-Response Relationship Between Daily Step Count and Health Outcomes: A Systematic Review and Meta-Analyses; CRD42021244747).…
PMID: 37676198
-
link
The association between daily step count and all-cause and cardiovascular mortality: a meta-analysis.
There is good evidence showing that inactivity and walking minimal steps/day increase the risk of cardiovascular (CV) disease and general ill-health. The optimal number of steps and their role in health is, however, still unclear. Therefore, in this meta-analysis, we aimed to evaluate the relationship between step count and all-cause mortality and CV mortality. We systematically searched relevant electronic databases from inception until 12 June 2022. The main endpoints were all-cause mortality and CV mortality. An inverse-variance weighted random-effects model was used to calculate the number of steps/day and mortality. Seventeen cohort studies with a total of 226 889 participants (generally healthy or patients at CV risk) with a median follow-up 7.1 years were included in the meta-analysis. A 1000-step increment was associated with a 15% decreased risk of all-cause mortality [hazard ratio (HR) 0.85; 95% confidence interval (CI) 0.81-0.91; P < 0.001], while a 500-step increment was associated with a 7% decrease in CV mortality (HR 0.93; 95% CI 0.91-0.95; P < 0.001). Compared with the reference quartile with median steps/day 3867 (2500-6675), the Quartile 1 (Q1, median steps: 5537), Quartile 2 (Q2, median steps 7370), and Quartile 3 (Q3, median steps 11 529) were associated with lower risk for all-cause mortality (48, 55, and 67%, respectively; P < 0.05, for all). Similarly, compared with the lowest quartile of steps/day used as reference [median steps 2337, interquartile range 1596-4000), higher quartiles of steps/day (Q1 = 3982, Q2 = 6661, and Q3 = 10 413) were linearly associated with a reduced risk of CV mortality (16, 49, and 77%; P < 0.05, for all). Using a restricted cubic splines model, we observed a nonlinear dose-response association between step count and all-cause and CV mortality (Pnonlineraly < 0.001, for both) with a progressively lower risk of mortality with an increased step count. This meta-analysis demonstrates a significant inverse association between daily step count and all-cause mortality and CV mortality with more the better over the cut-off point of 3867 steps/day for all-cause mortality and only 2337 steps for CV mortality. There is strong evidence showing that sedentary life may significantly increase the risk of cardiovascular (CV) disease and shorten the lifespan. However, the optimal number of steps, both the cut-off points over which we can see health benefits, and the upper limit (if any), and their role in health are still unclear. In this meta-analysis of 17 studies with almost 227 000 participants that assessed the health effects of physical activity expressed by walking measured in the number of steps, we showed that a 1000-step increment correlated with a significant reduction of all-cause mortality of 15%, and similarly, a 500-step increment correlated with a reduced risk of CV mortality of 7%. In addition, using the dose–response model, we observed a strong inverse nonlinear association between step count and all-cause mortality with significant differences between younger and older groups. It is the first analysis that not only looked at age and sex but also regional differences based on the weather zones, and for the first time, it assesses the effect of up to 20 000 steps/day on outcomes (confirming the more the better), which was missed in previous analyses. The analysis also revealed that depending on the outcomes, we do not need so many steps to have health benefits starting with even 2500/4000 steps/day, which, in fact, undermines the hitherto definition of a sedentary life.…
PMID: 37555441
"הסיכון לפגיעה במפרקים כתוצאה מהליכה מרובה גבוה יותר אם אין מסת שריר טובה שתגן על הגוף."
מסקנת הבדיקה:
הספרות המדעית מאשרת כי מסת שריר ותפקוד עצבי-שרירי תקין חיוניים להגנה על המפרקים, במיוחד בברכיים, ומסייעים בהפחתת העומס המכני המופעל עליהם במהלך הליכה. (🟩)
chevron_right מקורות מדעיים: (2)
-
link
The effect of body weight on the knee joint biomechanics based on subject-specific finite element-musculoskeletal approach.
Knee osteoarthritis (OA) and obesity are major public health concerns that are closely intertwined. This intimate relationship was documented by considering obesity as the most significant preventable risk factor associated with knee OA. To date, however, the effects of obesity on the knee joint's passive-active structure and cartilage loading have been inconclusive. Hence, this study investigates the intricate relationship between obesity and knee OA, centering on the biomechanical changes in knee joint active and passive reactions during the stance phase of gait. Using a subject-specific musculoskeletal and finite element approach, muscle forces, ligament stresses, and articular cartilage contact stresses were analyzed among 60 individuals with different body mass indices (BMI) classified under healthy weight, overweight, and obese categories. Our predicted results showed that obesity significantly influenced knee joint mechanical reaction, increasing muscle activations, ligament loading, and articular cartilage contact stresses, particularly during key instances of the gait cycle-first and second peak loading instances. The study underscores the critical role of excessive body weight in exacerbating knee joint stress distribution and cartilage damage. Hence, the insights gained provide a valuable biomechanical perspective on the interaction between body weight and knee joint health, offering a clinical utility in assessing the risks associated with obesity and knee OA.…
PMID: 38877075
-
link
The effects of a strength and neuromuscular exercise programme for the lower extremity on knee load, pain and function in obese children and adolescents: study protocol for a randomised controlled trial.
Childhood obesity is one of the most critical and accelerating health challenges throughout the world. It is a major risk factor for developing varus/valgus misalignments of the knee joint. The combination of misalignment at the knee and excess body mass may result in increased joint stresses and damage to articular cartilage. A training programme, which aims at developing a more neutral alignment of the trunk and lower limbs during movement tasks may be able to reduce knee loading during locomotion. Despite the large number of guidelines for muscle strength training and neuromuscular exercises that exist, most are not specifically designed to target the obese children and adolescent demographic. Therefore, the aim of this study is to evaluate a training programme which combines strength and neuromuscular exercises specifically designed to the needs and limitations of obese children and adolescents and analyse the effects of the training programme from a biomechanical and clinical point of view. A single assessor-blinded, pre-test and post-test randomised controlled trial, with one control and one intervention group will be conducted with 48 boys and girls aged between 10 and 18 years. Intervention group participants will receive a 12-week neuromuscular and quadriceps/hip strength training programme. Three-dimensional (3D) gait analyses during level walking and stair climbing will be performed at baseline and follow-up sessions. The primary outcome parameters for this study will be the overall peak external frontal knee moment and impulse during walking. Secondary outcomes include the subscales of the Knee injury and Osteoarthritis Outcome Score (KOOS), frontal and sagittal kinematics and kinetics for the lower extremities during walking and stair climbing, ratings of change in knee-related well-being, pain and function and adherence to the training programme. In addition, the training programme will be evaulated from a clinical and health status perspective by including the following analyses: cardiopulmonary testing to quantify aerobic fitness effects, anthropometric measures, nutritional status and psychological status to characterise the study sample. The findings will help to determine whether a neuromuscular and strength training exercise programme for the obese children population can reduce joint loading during locomotion, and thereby decrease the possible risk of developing degenerative joint diseases later in adulthood. ClinicalTrials NCT02545764 , Date of registration: 24 September 2015.…
PMID: 26700568

החדשות - N12
דירוג זה מבוסס על 1 דוחות אימות קודמים.
האם הדוח הזה היה מועיל לך?
מה היה פחות טוב? (רשות)
תודה על הפידבק!
עירעור על דוח זה
ספקו ראיות חדשות או הצביעו על אי דיוקים
נעדכן אותך על תוצאות הבדיקה
הוסיפו קישורים למחקרים או מקורות רפואיים מוכרים
העירעור נשלח בהצלחה!
המנוע המדעי שלנו יבדוק את הראיות שהגשתם. נעדכן אתכם באימייל עם התוצאות.
ניתוח מבוסס בינה מלאכותית
דוח זה נוצר באופן אוטומטי על ידי מערכת בינה מלאכותית ועשוי להכיל שגיאות, אי-דיוקים או מידע חלקי. הניתוח אינו מהווה ייעוץ רפואי, אבחנה או המלצה לטיפול, והוא אינו תחליף לדעתו של איש מקצוע רפואי מוסמך. יש להתייעץ עם רופא או מומחה מוסמך לפני קבלת כל החלטה רפואית. המידע מוצג לצרכי מידע כללי בלבד.
מידע זה מופק על ידי בינה מלאכותית ואינו מהווה תחליף לייעוץ רפואי מקצועי.