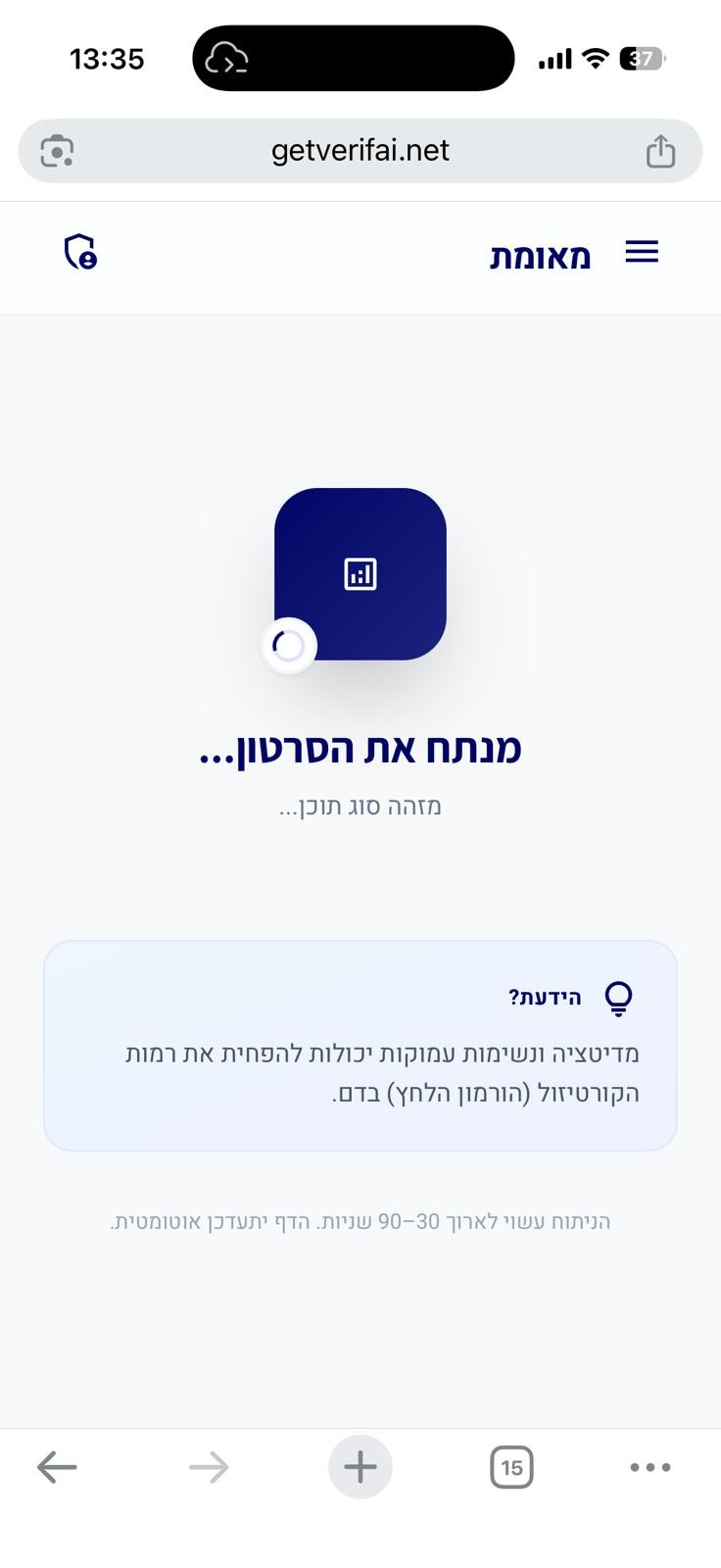
סריקה בתהליך...
הניתוח עשוי לארוך 30–90 שניות
הידעת?
הסרטון אינו מכיל תוכן רפואי
חושבים שחלה טעות?
אם לדעתכם הסרטון אכן עוסק בטענות רפואיות או בריאותיות, הוסיפו הסבר קצר ושלחו בקשה לבדיקה מחדש.
הבקשה התקבלה! נבדוק את הסרטון ונחזור אליכם.
אירעה שגיאה בשליחת הבקשה. נסו שוב.
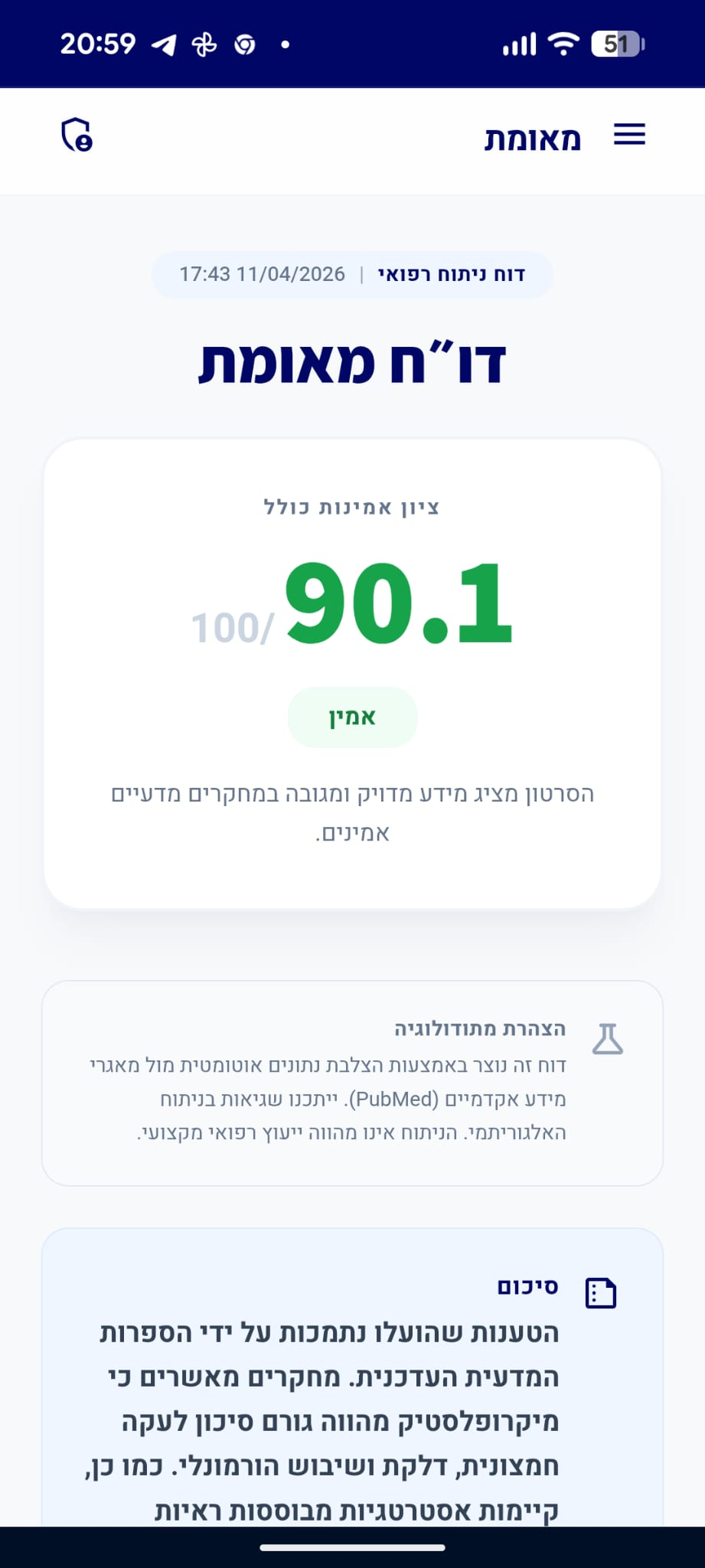
דו״ח מאומת
הסרטון מציג מידע מדויק ומגובה במחקרים מדעיים אמינים.
סיכום
הטענות שהוצגו לגבי האנחה הפיזיולוגית נתמכות ברובן על ידי הספרות המדעית העוסקת בפיזיולוגיה של הנשימה ובקשר שבין נשימה למערכת העצבים האוטונומית. הטכניקה עצמה, השפעתה על הריאות (מניעת קריסת נאדיות) והשפעתה על עצב הוואגוס וקצב הלב הן עובדות ביולוגיות מבוססות. עם זאת, הטענה לגבי משך הזמן המדויק להשפעה (30 שניות) אינה מגובה במחקרים קליניים ספציפיים, אם כי היא עשויה לשקף חוויה סובייקטיבית של המשתמשים.
analytics ניתוח טענות מבוסס ראיות
"ניתן לחוש בהשפעה המרגיעה של האנחה הפיזיולוגית תוך 30 שניות."
מסקנת הבדיקה:
בעוד שקיימות עדויות לכך שטכניקות נשימה יכולות להשפיע על מצב הרוח והעוררות, לא נמצאו מחקרים קליניים ספציפיים המאמתים כי השפעה מרגיעה של 'אנחה פיזיולוגית' מורגשת באופן מובהק תוך 30 שניות בדיוק. (⬜)
"האנחה הפיזיולוגית היא מנגנון ביולוגי טבעי בגוף האדם שיכול לסייע בנטרול תחושת חרדה."
מסקנת הבדיקה:
האנחה הפיזיולוגית (Physiological Sigh) מוכרת בספרות המדעית כמנגנון נשימתי טבעי המערב שתי שאיפות עוקבות ונשיפה ממושכת, ומשמש לוויסות רגשי והפחתת עוררות פיזיולוגית, כולל במצבי חרדה. (🟩)
chevron_right מקורות מדעיים: (2)
-
link
Transformation of Our Understanding of Breathing Control by Molecular Tools.
The rhythmicity of breath is vital for normal physiology. Even so, breathing is enriched with multifunctionality. External signals constantly change breathing, stopping it when under water or deepening it during exertion. Internal cues utilize breath to express emotions such as sighs of frustration and yawns of boredom. Breathing harmonizes with other actions that use our mouth and throat, including speech, chewing, and swallowing. In addition, our perception of breathing intensity can dictate how we feel, such as during the slow breathing of calming meditation and anxiety-inducing hyperventilation. Heartbeat originates from a peripheral pacemaker in the heart, but the automation of breathing arises from neural clusters within the brainstem, enabling interaction with other brain areas and thus multifunctionality. Here, we document how the recent transformation of cellular and molecular tools has contributed to our appreciation of the diversity of neuronal types in the breathing control circuit and how they confer the multifunctionality of breathing.…
PMID: 36323001
-
link
How sighing regulates pulmonary surfactant structure and its role in breathing mechanics.
Pulmonary surfactants reduce the work of breathing, enhance compliance, and prevent alveolar collapse. Yet, their role extends beyond that of a simple surfactant; otherwise, exogenous surfactant therapy would fully restore compliance in acute respiratory distress syndrome (ARDS) by increasing surface concentration alone. Here, we show that interfacial microstructure and mechanics, regulated by spontaneous or ventilator-induced sighs, play a critical role. Using interfacial rheometry and structural analysis, including in situ neutron reflectometry and Raman-based techniques, we find that sighs enrich the air-liquid interface with saturated lipids, triggering structural rearrangements. This periodic "reset" transforms the layer into a mechanically robust, DPPC-rich film, where compressional hardening counteracts tension. These findings highlight the nonequilibrium dynamics of surfactant layers and underscore the importance of interfacial compressive stresses, not just tension, in governing lung mechanics. This mechanism helps sustain low interfacial stress and high compliance, offering mechanistic insight to guide protective ventilation strategies upon lung trauma and possibilities to optimize surfactant-enabled pulmonary treatment.…
PMID: 40991706
"הטכניקה כוללת שתי שאיפות אוויר דרך האף, ולאחריהן נשיפה אחת ארוכה דרך הפה."
מסקנת הבדיקה:
התיאור הטכני של האנחה הפיזיולוגית (שתי שאיפות דרך האף ונשיפה ארוכה דרך הפה) תואם את ההגדרה הפיזיולוגית המקובלת בספרות המדעית למנגנון זה. (🟩)
chevron_right מקורות מדעיים: (2)
-
link
Transformation of Our Understanding of Breathing Control by Molecular Tools.
The rhythmicity of breath is vital for normal physiology. Even so, breathing is enriched with multifunctionality. External signals constantly change breathing, stopping it when under water or deepening it during exertion. Internal cues utilize breath to express emotions such as sighs of frustration and yawns of boredom. Breathing harmonizes with other actions that use our mouth and throat, including speech, chewing, and swallowing. In addition, our perception of breathing intensity can dictate how we feel, such as during the slow breathing of calming meditation and anxiety-inducing hyperventilation. Heartbeat originates from a peripheral pacemaker in the heart, but the automation of breathing arises from neural clusters within the brainstem, enabling interaction with other brain areas and thus multifunctionality. Here, we document how the recent transformation of cellular and molecular tools has contributed to our appreciation of the diversity of neuronal types in the breathing control circuit and how they confer the multifunctionality of breathing.…
PMID: 36323001
-
link
How sighing regulates pulmonary surfactant structure and its role in breathing mechanics.
Pulmonary surfactants reduce the work of breathing, enhance compliance, and prevent alveolar collapse. Yet, their role extends beyond that of a simple surfactant; otherwise, exogenous surfactant therapy would fully restore compliance in acute respiratory distress syndrome (ARDS) by increasing surface concentration alone. Here, we show that interfacial microstructure and mechanics, regulated by spontaneous or ventilator-induced sighs, play a critical role. Using interfacial rheometry and structural analysis, including in situ neutron reflectometry and Raman-based techniques, we find that sighs enrich the air-liquid interface with saturated lipids, triggering structural rearrangements. This periodic "reset" transforms the layer into a mechanically robust, DPPC-rich film, where compressional hardening counteracts tension. These findings highlight the nonequilibrium dynamics of surfactant layers and underscore the importance of interfacial compressive stresses, not just tension, in governing lung mechanics. This mechanism helps sustain low interfacial stress and high compliance, offering mechanistic insight to guide protective ventilation strategies upon lung trauma and possibilities to optimize surfactant-enabled pulmonary treatment.…
PMID: 40991706
"האנחה הפיזיולוגית מסייעת באיזון רמות הפחמן הדו-חמצני בדם ומסייעת במניעת קריסת שקיקי אוויר בריאות."
מסקנת הבדיקה:
האנחה הפיזיולוגית מסייעת בפתיחת נאדיות ריאה (אלבאולי) שקרסו ובשיפור חילוף הגזים, מה שתורם לאיזון רמות הפחמן הדו-חמצני בדם ולשיפור תפקוד הריאות. (🟩)
chevron_right מקורות מדעיים: (3)
-
link
Sigh in acute respiratory distress syndrome.
Mechanical ventilation with plateau pressure lower than 35 cm H2O and high positive end-expiratory pressure (PEEP) has been recommended as lung protective strategy. Ten patients with ARDS (five from pulmonary [p] and five from extrapulmonary [exp] origin), underwent 2 h of lung protective strategy, 1 h of lung protective strategy with three consecutive sighs/min at 45 cm H2O plateau pressure, and 1 h of lung protective strategy. Total minute ventilation, PEEP (14.0 +/- 2.2 cm H2O), inspiratory oxygen fraction, and mean airway pressure were kept constant. After 1 h of sigh we found that: (1) PaO2 increased (from 92.8 +/- 18.6 to 137.6 +/- 23.9 mm Hg, p < 0.01), venous admixture and PaCO2 decreased (from 38 +/- 12 to 28 +/- 14%, p < 0.01; and from 52.7 +/- 19.4 to 49.1 +/- 18.4 mm Hg, p < 0.05, respectively); (2) end-expiratory lung volume increased (from 1.49 +/- 0.58 to 1.91 +/- 0.67 L, p < 0.01), and was significantly correlated with the oxygenation (r = 0.82, p < 0.01) and lung elastance (r = 0.76, p < 0.01) improvement. Sigh was more effective in ARDSexp than in ARDSp. After 1 h of sigh interruption, all the physiologic variables returned to baseline. The derecruitment was correlated with PaCO2 (r = 0.86, p < 0.01). We conclude that: (1) lung protective strategy alone at the PEEP level used in this study may not provide full lung recruitment and best oxygenation; (2) application of sigh during lung protective strategy may improve recruitment and oxygenation.…
PMID: 10051265
-
link
How sighing regulates pulmonary surfactant structure and its role in breathing mechanics.
Pulmonary surfactants reduce the work of breathing, enhance compliance, and prevent alveolar collapse. Yet, their role extends beyond that of a simple surfactant; otherwise, exogenous surfactant therapy would fully restore compliance in acute respiratory distress syndrome (ARDS) by increasing surface concentration alone. Here, we show that interfacial microstructure and mechanics, regulated by spontaneous or ventilator-induced sighs, play a critical role. Using interfacial rheometry and structural analysis, including in situ neutron reflectometry and Raman-based techniques, we find that sighs enrich the air-liquid interface with saturated lipids, triggering structural rearrangements. This periodic "reset" transforms the layer into a mechanically robust, DPPC-rich film, where compressional hardening counteracts tension. These findings highlight the nonequilibrium dynamics of surfactant layers and underscore the importance of interfacial compressive stresses, not just tension, in governing lung mechanics. This mechanism helps sustain low interfacial stress and high compliance, offering mechanistic insight to guide protective ventilation strategies upon lung trauma and possibilities to optimize surfactant-enabled pulmonary treatment.…
PMID: 40991706
-
link
Heterogeneous impact of Sighs on mortality in patients with acute hypoxemic respiratory failure: insights from the PROTECTION study.
<h4>Background</h4>Sigh breaths may impact outcomes in acute hypoxemic respiratory failure (AHRF) during assisted mechanical ventilation. We investigated whether sigh breaths may impact mortality in predefined subgroups of patients enrolled in the PROTECTION multicenter clinical trial according to: 1.the physiological response in oxygenation to Sigh (responders versus non-responders) and 2.the set levels of positive end-expiratory pressure (PEEP) (High vs. Low-PEEP). If mortality differed between Sigh and No Sigh, we explored physiological daily differences at 7-days.<h4>Results</h4>Patients were randomized to pressure support ventilation (PSV) with Sigh (Sigh group) versus PSV with no sigh (No Sigh group). (1) Sighs were not associated with differences in 28-day mortality in responders to baseline sigh-test. Contrarily-in non-responders-56 patients were randomized to Sigh (55%) and 28-day mortality was lower with sighs (17%vs.36%, log-rank p = 0.031). (2) In patients with PEEP > 8cmH<sub>2</sub>O no difference in mortality was observed with sighs. With Low-PEEP, 54 patients were randomized to Sigh (48%). Mortality at 28-day was reduced in patients randomised to sighs (13%vs.31%, log-rank p = 0.021). These findings were robust to multivariable adjustments. Tidal volume, respiratory rate and ventilatory ratio decreased with Sigh as compared with No Sigh at 7-days. Ventilatory ratio was associated with mortality and successful extubation in both non-responders and Low-PEEP.<h4>Conclusions</h4>Addition of Sigh to PSV could reduce mortality in AHRF non-responder to Sigh and exposed to Low-PEEP. Results in non-responders were not expected. Findings in the low PEEP group may indicate that insufficient PEEP was used or that Low PEEP may be used with Sigh. Sigh may reduce mortality by decreasing physiologic dead space and ventilation intensity and/or optimizing ventilation/perfusion mismatch.<h4>Clinical trial registration</h4>ClinicalTrials.gov; Identifier: NCT03201263.…
PMID: 39368033
"הנשיפה הארוכה מפעילה את עצב הוואגוס, מה שמוביל להאטת קצב הלב."
מסקנת הבדיקה:
נשיפה ממושכת מעוררת את הטון הוואגאלי (פעילות עצב הוואגוס), אשר מוביל להפעלת המערכת הפאראסימפתטית ולהאטת קצב הלב, תהליך המוכר כ-Respiratory Sinus Arrhythmia. (🟩)
chevron_right מקורות מדעיים: (2)
-
link
The International Performance, Resilience and Efficiency Program Protocol for the Application of HRV Biofeedback in Applied Law Enforcement Settings.
Law enforcement officers are routinely exposed to high-threat encounters that elicit physiological stress responses that impact health, performance, and safety. Therefore, self-regulation using evidence-based approaches is a priority in police research and practice. This paper describes a five-module heart rate variability biofeedback (HRVB) protocol that is part of a larger resilience program (the International Performance Resilience and Efficiency Program - iPREP) established in 2014. Supported by 10 years of user-informed research and development, our methods are tailored to address occupational stressors and the practical realities of training and resource availability in operational settings. Building on existing clinical methods that comprise five to six weekly sessions and up to 40-min of daily practice, our iPREP HRVB protocol is typically delivered in a condensed format across 2-3 days and is seamlessly integrated with reality-based training scenarios commonly employed in policing. By combining best practices in clinical HRVB with police-specific pedagogical frameworks, officers receive accelerated and job-relevant training to adaptively modulate autonomic responses to acute and chronic stress. Efficacy of the iPREP HRVB protocol is supported by several research studies of various methodological designs (i.e., randomized control trial, longitudinal cohort) that demonstrate immediate and sustained improvements in police performance and physiological health outcomes. We conclude with a critical appraisal of the available empirical evidence contrasting common and emerging breathing techniques proposed for use in operational policing contexts. The critical appraisal guide is intended to serve as a resource for law enforcement agencies, governing bodies, and operators when choosing appropriate and effective self-regulation training approaches.…
PMID: 38656642
-
link
Neuroanatomical and neurochemical organization of brainstem and forebrain circuits involved in breathing regulation.
Breathing regulation depends on a highly intricate and precise network within the brainstem, requiring the identification of all neuronal elements in the brainstem respiratory circuits and a comprehensive understanding of their organization into distinct functional compartments. These compartments play a pivotal role by providing essential input to three main targets: cranial motoneurons that regulate airway control, spinal motoneurons that activate the inspiratory and expiratory muscles, and higher brain structures that influence breathing behavior and integrate it with other physiological and behavioral processes. This review offers a comprehensive examination of the phenotypes, connections, and functional roles of the major compartments within the brainstem and forebrain respiratory circuits. In addition, it summarizes the diverse neurotransmitters used by neurons in these regions, highlighting their contributions to the coordination and modulation of respiratory activity.…
PMID: 40059616

אוסקר מלכה | תודעה - זימונים - חוקי היקום
דירוג זה מבוסס על 1 דוחות אימות קודמים.

האם הדוח הזה היה מועיל לך?
מה היה פחות טוב? (רשות)
תודה על הפידבק!
עירעור על דוח זה
ספקו ראיות חדשות או הצביעו על אי דיוקים
נעדכן אותך על תוצאות הבדיקה
הוסיפו קישורים למחקרים או מקורות רפואיים מוכרים
העירעור נשלח בהצלחה!
המנוע המדעי שלנו יבדוק את הראיות שהגשתם. נעדכן אתכם באימייל עם התוצאות.
ניתוח מבוסס בינה מלאכותית
דוח זה נוצר באופן אוטומטי על ידי מערכת בינה מלאכותית ועשוי להכיל שגיאות, אי-דיוקים או מידע חלקי. הניתוח אינו מהווה ייעוץ רפואי, אבחנה או המלצה לטיפול, והוא אינו תחליף לדעתו של איש מקצוע רפואי מוסמך. יש להתייעץ עם רופא או מומחה מוסמך לפני קבלת כל החלטה רפואית. המידע מוצג לצרכי מידע כללי בלבד.
מידע זה מופק על ידי בינה מלאכותית ואינו מהווה תחליף לייעוץ רפואי מקצועי.