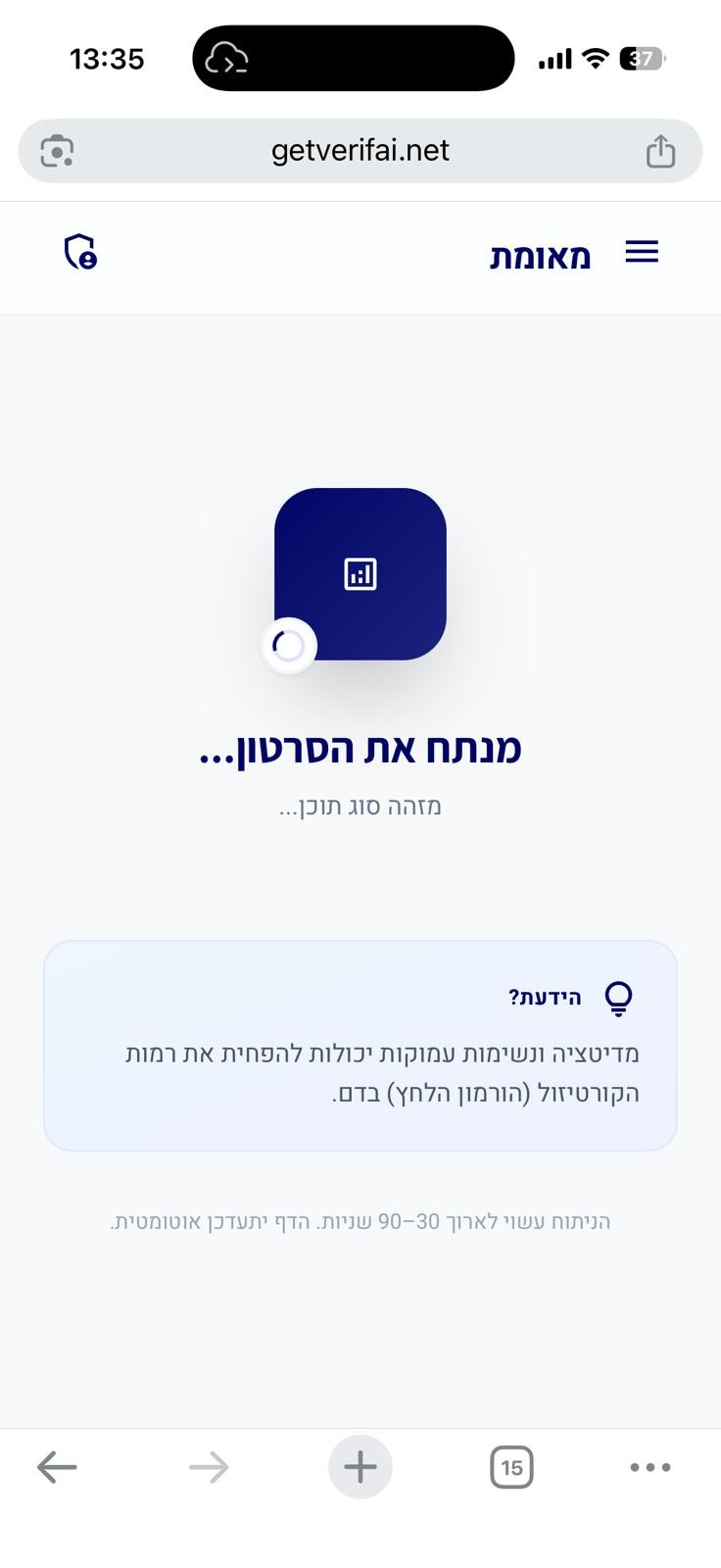
סריקה בתהליך...
הניתוח עשוי לארוך 30–90 שניות
הידעת?
הסרטון אינו מכיל תוכן רפואי
חושבים שחלה טעות?
אם לדעתכם הסרטון אכן עוסק בטענות רפואיות או בריאותיות, הוסיפו הסבר קצר ושלחו בקשה לבדיקה מחדש.
הבקשה התקבלה! נבדוק את הסרטון ונחזור אליכם.
אירעה שגיאה בשליחת הבקשה. נסו שוב.
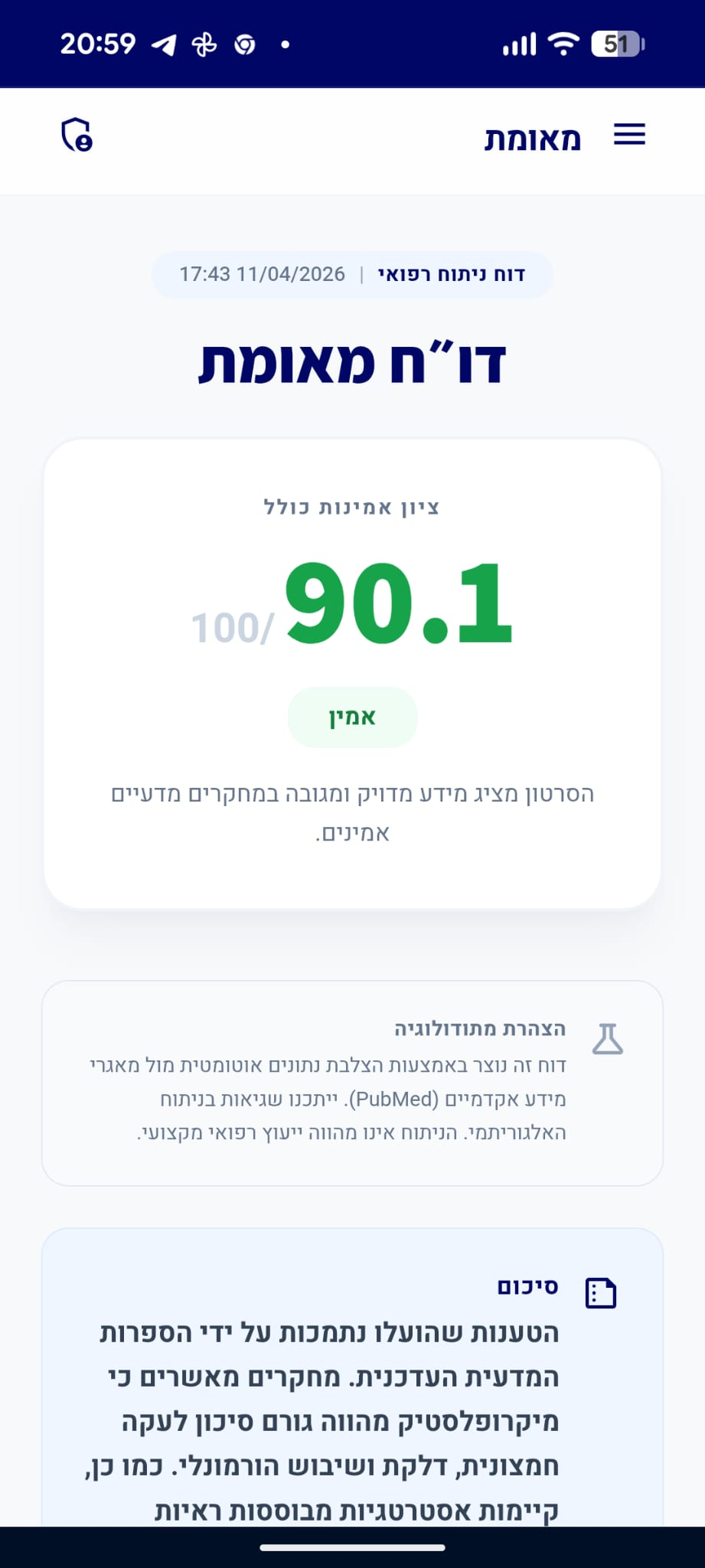
דו״ח מאומת
הסרטון מציג מידע מדויק ומגובה במחקרים מדעיים אמינים.
סיכום
הטענות שהועלו בסרטון עולות בקנה אחד עם הידע המדעי העדכני. אין בסיס מדעי לשיטות 'ניקוי רעלים' או לייחוס סגולות ריפוי מיוחדות ללימון בהקשר של תפקוד הכבד או מניעת סרטן.
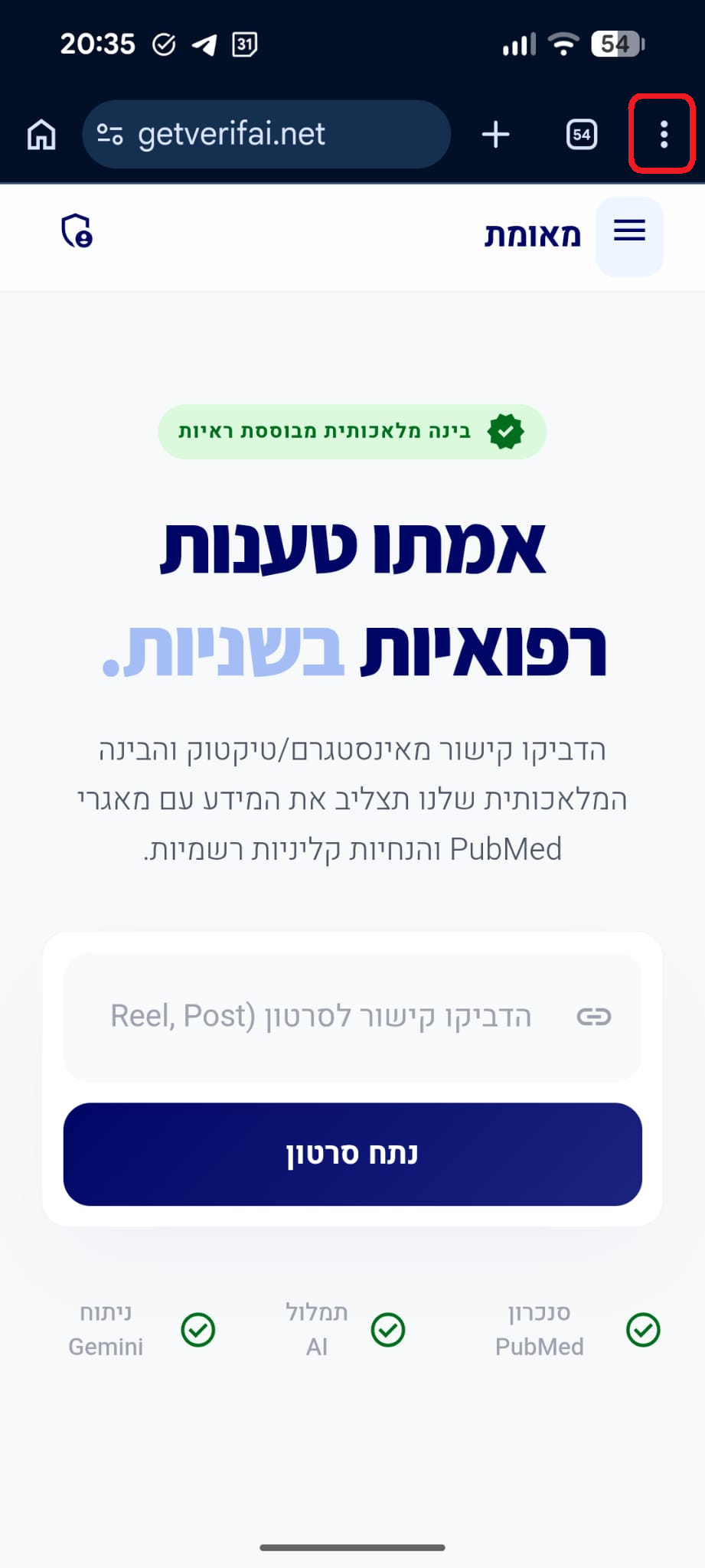
analytics ניתוח טענות מבוסס ראיות
"סרטן נגרם משינויים גנטיים בתאים ויכול להתפתח כמעט בכל איבר בגוף."
מסקנת הבדיקה:
סרטן אכן נגרם ממוטציות גנטיות ושינויים בתאים, והוא יכול להתפתח במגוון רחב של איברים בגוף כתוצאה מתהליכים אלו. (🟩)
chevron_right מקורות מדעיים: (3)
-
link
[Carcinogenesis].
Cell division is controlled by stimulatory and inhibitory systems.The origin of cancer is monoclonal, and in order that a normal cell switches its phenotype and becomes a neoplastic cell, genetic mutations must occur on it.These genetic mutations modify the products that in normal conditions the gene would codify and, finally, cause cancer. Cancer may be hereditary (due to mutations in one or both of germinal cells alleles) or sporadic (due to action of environmental mutagenic agents).The mechanisms that may cause alterations on genes may be genetic or epigenetic. Genetic mechanisms occur when structural alterations of genome are present and the epigenetic processes occur due to enzymatic alterations or alterations on its substrates. Carcinogenesis has three stages: initiation, promotion and progression.The last of these stages, progression, is exclusive of malignant transformation and implies the capacity to invade surrounding or distant tissues. For metastasis to take place, many mechanisms are required: angiogenesis, matrix degradation, cell migration, evasion of host immune response and metastatic colonization. This article presents a partial review of current bibliography about concepts related to carcinogenesis and conveys the minimum necessary information to achieve an understanding of this complex process.…
PMID: 22218794
-
link
Cancers make their own luck: theories of cancer origins.
Cancer has been a leading cause of death for decades. This dismal statistic has increased efforts to prevent the disease or to detect it early, when treatment is less invasive, relatively inexpensive and more likely to cure. But precisely how tissues are transformed continues to provoke controversy and debate, hindering cancer prevention and early intervention strategies. Various theories of cancer origins have emerged, including the suggestion that it is 'bad luck': the inevitable consequence of random mutations in proliferating stem cells. In this Review, we discuss the principal theories of cancer origins and the relative importance of the factors that underpin them. The body of available evidence suggests that developing and ageing tissues 'walk a tightrope', retaining adequate levels of cell plasticity to generate and maintain tissues while avoiding overstepping into transformation. Rather than viewing cancer as 'bad luck', understanding the complex choreography of cell intrinsic and extrinsic factors that characterize transformation holds promise to discover effective new ways to prevent, detect and stop cancer before it becomes incurable.…
PMID: 37488363
-
link
Stem cells, cancer, and cancer stem cells.
Stem cell biology has come of age. Unequivocal proof that stem cells exist in the haematopoietic system has given way to the prospective isolation of several tissue-specific stem and progenitor cells, the initial delineation of their properties and expressed genetic programmes, and the beginnings of their utility in regenerative medicine. Perhaps the most important and useful property of stem cells is that of self-renewal. Through this property, striking parallels can be found between stem cells and cancer cells: tumours may often originate from the transformation of normal stem cells, similar signalling pathways may regulate self-renewal in stem cells and cancer cells, and cancer cells may include 'cancer stem cells' - rare cells with indefinite potential for self-renewal that drive tumorigenesis.…
PMID: 11689955
"אין ראיות מדעיות לכך שלימון מגן מפני סרטן או משפר את תפקוד הכבד."
מסקנת הבדיקה:
אין ראיות קליניות מבוססות לכך ששתיית מים עם לימון מונעת סרטן או משפרת את תפקוד הכבד. הכבד מתפקד באופן עצמאי ללא קשר לצריכת לימון. (🟩)
"הכבד אינו שריר, אלא איבר הפועל באמצעות תהליכים ביוכימיים מורכבים."
מסקנת הבדיקה:
הכבד הוא איבר בלוטי המבצע תהליכים ביוכימיים מורכבים (כמו מטבוליזם וסינון) ואינו שריר בעל יכולת התכווצות. (🟩)
chevron_right מקורות מדעיים: (2)
-
link
Spatial heterogeneity in the mammalian liver.
Hepatocytes operate in highly structured repeating anatomical units termed liver lobules. Blood flow along the lobule radial axis creates gradients of oxygen, nutrients and hormones, which, together with morphogenetic fields, give rise to a highly variable microenvironment. In line with this spatial variability, key liver functions are expressed non-uniformly across the lobules, a phenomenon termed zonation. Technologies based on single-cell transcriptomics have constructed a global spatial map of hepatocyte gene expression in mice revealing that ~50% of hepatocyte genes are expressed in a zonated manner. This broad spatial heterogeneity suggests that hepatocytes in different lobule zones might have not only different gene expression profiles but also distinct epigenetic features, regenerative capacities, susceptibilities to damage and other functional aspects. Here, we present genomic approaches for studying liver zonation, describe the principles of liver zonation and discuss the intrinsic and extrinsic factors that dictate zonation patterns. We also explore the challenges and solutions for obtaining zonation maps of liver non-parenchymal cells. These approaches facilitate global characterization of liver function with high spatial resolution along physiological and pathological timescales.…
PMID: 30936469
-
link
Spatial metabolomics and its application in the liver.
Hepatocytes work in highly structured, repetitive hepatic lobules. Blood flow across the radial axis of the lobule generates oxygen, nutrient, and hormone gradients, which result in zoned spatial variability and functional diversity. This large heterogeneity suggests that hepatocytes in different lobule zones may have distinct gene expression profiles, metabolic features, regenerative capacity, and susceptibility to damage. Here, we describe the principles of liver zonation, introduce metabolomic approaches to study the spatial heterogeneity of the liver, and highlight the possibility of exploring the spatial metabolic profile, leading to a deeper understanding of the tissue metabolic organization. Spatial metabolomics can also reveal intercellular heterogeneity and its contribution to liver disease. These approaches facilitate the global characterization of liver metabolic function with high spatial resolution along physiological and pathological time scales. This review summarizes the state of the art for spatially resolved metabolomic analysis and the challenges that hinder the achievement of metabolome coverage at the single-cell level. We also discuss several major contributions to the understanding of liver spatial metabolism and conclude with our opinion on the future developments and applications of these exciting new technologies.…
PMID: 36811413
"המושג 'כבד עמוס רעלים' אינו קיים ברפואה; כשל בפירוק חומרים מעיד על מחלת כבד."
מסקנת הבדיקה:
ברפואה הקונבנציונלית אין מושג של 'כבד עמוס רעלים'. פגיעה ביכולת הפירוק של הכבד מעידה על מחלת כבד ספציפית ולא על צורך ב'ניקוי'. (🟩)
chevron_right מקורות מדעיים: (2)
-
link
Myths and facts about the role of diet in metabolic dysfunction-associated steatotic liver disease.
Metabolic dysfunction-associated steatotic liver disease (MASLD) has become a leading cause of liver-related morbidity worldwide. Despite broad consensus on the importance of diet in managing the disease, numerous myths and misconceptions persist among patients, healthcare professionals, and the general public. This article aims to critically review the main myths and facts surrounding the role of diet in MASLD, in light of the most current scientific evidence.…
PMID: 40901600
-
link
Neonatal cholestasis is associated with cytochrome P450 1A2 detoxification defect: A single center pilot study.
<h4>Background</h4>Evidence supports that biliary atresia (BA) in Egyptian infants is an aflatoxin-induced cholangiopathy acquired perinatally in infants with glutathione S-transferase M1 deficiency: The Kotb disease BA variant. This inability to detoxify aflatoxins leads to progressive inflammatory adhesions and obliterative cholangiopathy early in life.<h4>Aim</h4>To investigate the cytochrome P450 1A2 (CYP1A2) detoxification enzyme levels in neonates with confirmed BA.<h4>Methods</h4>This prospective descriptive analytical study estimated CYP1A2 detoxification enzyme levels using enzyme-linked immunosorbent assay in 20 neonates with confirmed BA. The level CYP1A2 was also estimated in a control group of 20 infants with neonatal hepatitis (NH) and 20 age- and sex-matched healthy infants.<h4>Results</h4>The mean age at enrollment in the study was 2.16 ± 0.58 months, 2.51 ± 1.05 months and 1.9 ± 0.81 months for the BA, NH and control group (<i>P</i> = 0.42). The mean ± SD of CYP1A2 among BA, NH and control group was 13.58 ± 9.73, 9.59 ± 9.95 and 31.68 ± 12.33 (<i>P</i> = 0.001). Within 3 months of follow up, of those with BA who underwent portoenterostomy 12 (60%) had successful outcome and cleared the jaundice, 5 (25%) had a stationary course and did not clear the jaundice while 3 (15%) died. The cholestasis resolved in 5 (25%) of the NH group, and improved in 15 (75%). CYP1A2 level did not correlate with age (<i>r</i> = 0.1559, <i>P</i> = 0.336), or total bilirubin level (<i>r</i> = 0.156, <i>P</i> = 0.336), alanine aminotransferase (<i>r</i> = -0.166, <i>P</i> = 0.305), aspartate aminotransferase (<i>r</i> = 0.091, <i>P</i> = 0.576), gamma glutamyl transferase (<i>r</i> = -0.0027, <i>P</i> = 0.99), alkaline phosphatase (<i>r</i> = 0.1059, <i>P</i> = 0.515), or outcome (<i>r</i> = 1.565, <i>P</i> = 0.23). A low CYP1A2 predicted a susceptibility to cholestasis by logistic regression (<i>P</i> = 0.000, 95% confidence interval: 0.8224-0.9327).<h4>Conclusion</h4>Significantly low serum CYP1A2 was frequent among infants with BA and NH compared to the control group. The low serum CYP1A2 compromises the detoxification ability of neonates with cholestasis and may alter the pharmacokinetics of commonly used drugs. Careful consideration to drug dosing and toxicity risk should be given to those neonates. Further research on drug pharmacokinetics and detoxification in neonates with cholestasis is recommended.…
PMID: 41884039
"כאבי ראש ומיגרנות אינם סימן לניקוי רעלים מהגוף."
מסקנת הבדיקה:
כאבי ראש ומיגרנות הם מצבים נוירולוגיים עם גורמים גנטיים, מטבוליים וסביבתיים, ואינם תסמין של 'ניקוי רעלים' מהגוף. (🟩)
chevron_right מקורות מדעיים: (2)
-
link
Chronic migraine: comorbidities, risk factors, and rehabilitation.
Migraine is a serious illness with a spontaneous clinical evolution into a chronic form. In some episodic migraines, increase of crises frequency modifies the headache pattern in the chronic form, defined as chronic migraine (CM), with headache frequency of 15 days/month. One-year prevalence of CM includes around 2-4% of the general population. Migraine progression from episodic to chronic form is realized through a period of time involving several months or years, during which an increase of attack frequency occurs. Migraine shows a wide spectrum of comorbidities, including cardiocerebral, vascular, psychiatric, metabolic, neurologic as well as other pathologies. The single/multiple presence of such comorbidities represents a fixed factor in the process of chronicization into CM. Risk factors including medication overuse headache (MOH), obesity, and lifestyle cooperate in the evolution process to CM. MOH is the most severe complication of CM, and similarly to CM its appearance is gradual. Both CM and MOH show particular genetic background able to favor the appearance of chronicity and abuse. Rehabilitation consists of drug withdrawal procedures, re-prophylaxis through administration of innovative drugs, such as OnabotulinumtoxinA and/or topiramate, to avoid relapsing attacks, and behavioral strategies to minimize the role of risk factors. The initial relief step for drug abusers always relies in drug withdrawal. The feasible diagnostic setting for a CM tailored treatment based on the application of pharmacogenomics will allow us to predetermine the efficacy of single old and new drugs by avoiding abuse due to non-responsivity of the acute drug.…
PMID: 20865469
-
link
Metabolic Dysfunction and Dietary Interventions in Migraine Management: The Role of Insulin Resistance and Neuroinflammation-A Narrative and Scoping Review.
<h4>Introduction</h4>Migraine is a prevalent neurological disorder characterized by recurrent headaches with autonomic and neurological symptoms, significantly impacting quality of life globally. Its pathogenesis involves genetic, neurological, inflammatory, and metabolic factors, with insulin resistance and metabolic dysfunction increasingly recognized as important contributors. Historically, it has been known that certain foods can trigger migraine attacks, which led for many years to the recommendation of elimination diets-now understood to primarily target histamine-rich foods. Over the past two decades, attention has shifted toward underlying metabolic disturbances, leading to the development of dietary approaches specifically aimed at addressing these dysfunctions.<h4>Methods</h4>A scoping literature review was conducted using PubMed and Embase to evaluate the relationships among migraine, insulin-related mechanisms, neurogenic inflammation, and dietary interventions. Initial searches focused on "MIGRAINE AND (neurogenic inflammation)" (2019-15 April 2025), followed by expanded searches from 1950 onward using terms such as "MIGRAINE AND (insulin, insulin resistance, hyperinsulinism)", and "MIGRAINE AND (diet, dietary, nutrition, nutritional)". A specific search also targeted "(INSULIN OR insulin resistance OR hyperinsulinism) AND (neurogenic inflammation)". Abstracts were screened, full texts were retrieved, and duplicates or irrelevant publications were excluded. No filters were applied by article type or language. Systematic reviews and meta-analyses were prioritized when available.<h4>Results</h4>Migraine pathogenesis involves trigeminovascular system activation, neurogenic inflammation mediated by CGRP and PACAP, immune dysregulation, mast cell activation, and cortical spreading depression (CSD). Emerging evidence highlights significant associations between migraine, insulin resistance, and hyperinsulinism. Hyperinsulinism contributes to migraine through TRPV1 sensitization, increased CGRP release, oxidative stress, mitochondrial dysfunction, and systemic inflammation. Metabolic dysfunction, including obesity and insulin resistance, exacerbates migraine severity and frequency. Dietary interventions, particularly anti-inflammatory, Mediterranean, and ketogenic diets, show promise in reducing migraine frequency and severity through mechanisms involving reduced inflammation, oxidative stress, improved mitochondrial function, and glucose metabolism stabilization.<h4>Conclusions</h4>The interplay between insulin resistance, metabolic dysfunction, and neuroinflammation is crucial in migraine pathophysiology. Targeted dietary interventions, including ketogenic and Mediterranean diets, demonstrate significant potential in managing migraines, emphasizing the need for personalized nutritional strategies to optimize therapeutic outcomes.…
PMID: 40426647

Inna Kreinin Bleicher
דירוג זה מבוסס על 2 דוחות אימות קודמים.

האם הדוח הזה היה מועיל לך?
מה היה פחות טוב? (רשות)
תודה על הפידבק!
עירעור על דוח זה
ספקו ראיות חדשות או הצביעו על אי דיוקים
נעדכן אותך על תוצאות הבדיקה
הוסיפו קישורים למחקרים או מקורות רפואיים מוכרים
העירעור נשלח בהצלחה!
המנוע המדעי שלנו יבדוק את הראיות שהגשתם. נעדכן אתכם באימייל עם התוצאות.
ניתוח מבוסס בינה מלאכותית
דוח זה נוצר באופן אוטומטי על ידי מערכת בינה מלאכותית ועשוי להכיל שגיאות, אי-דיוקים או מידע חלקי. הניתוח אינו מהווה ייעוץ רפואי, אבחנה או המלצה לטיפול, והוא אינו תחליף לדעתו של איש מקצוע רפואי מוסמך. יש להתייעץ עם רופא או מומחה מוסמך לפני קבלת כל החלטה רפואית. המידע מוצג לצרכי מידע כללי בלבד.
מידע זה מופק על ידי בינה מלאכותית ואינו מהווה תחליף לייעוץ רפואי מקצועי.