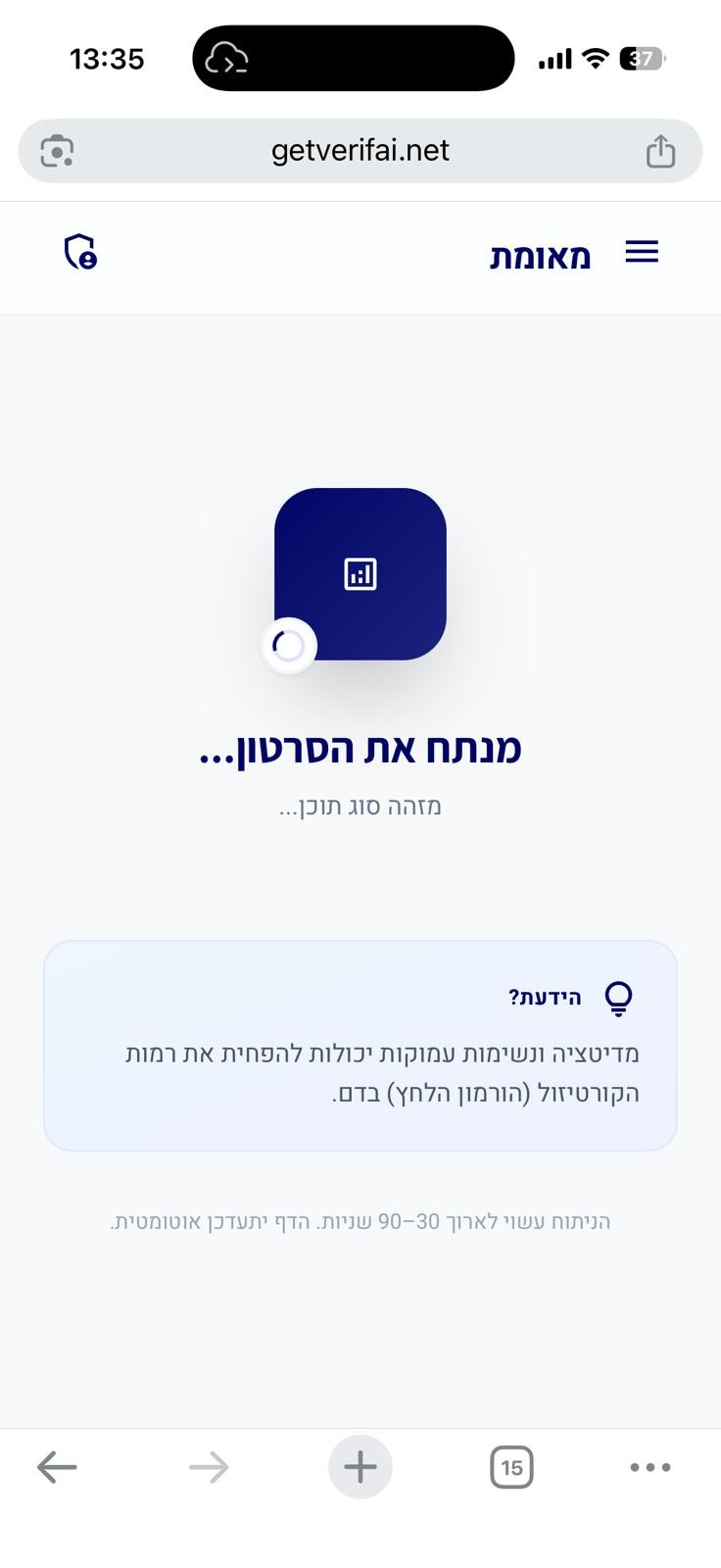
סריקה בתהליך...
הניתוח עשוי לארוך 30–90 שניות
הידעת?
הסרטון אינו מכיל תוכן רפואי
חושבים שחלה טעות?
אם לדעתכם הסרטון אכן עוסק בטענות רפואיות או בריאותיות, הוסיפו הסבר קצר ושלחו בקשה לבדיקה מחדש.
הבקשה התקבלה! נבדוק את הסרטון ונחזור אליכם.
אירעה שגיאה בשליחת הבקשה. נסו שוב.
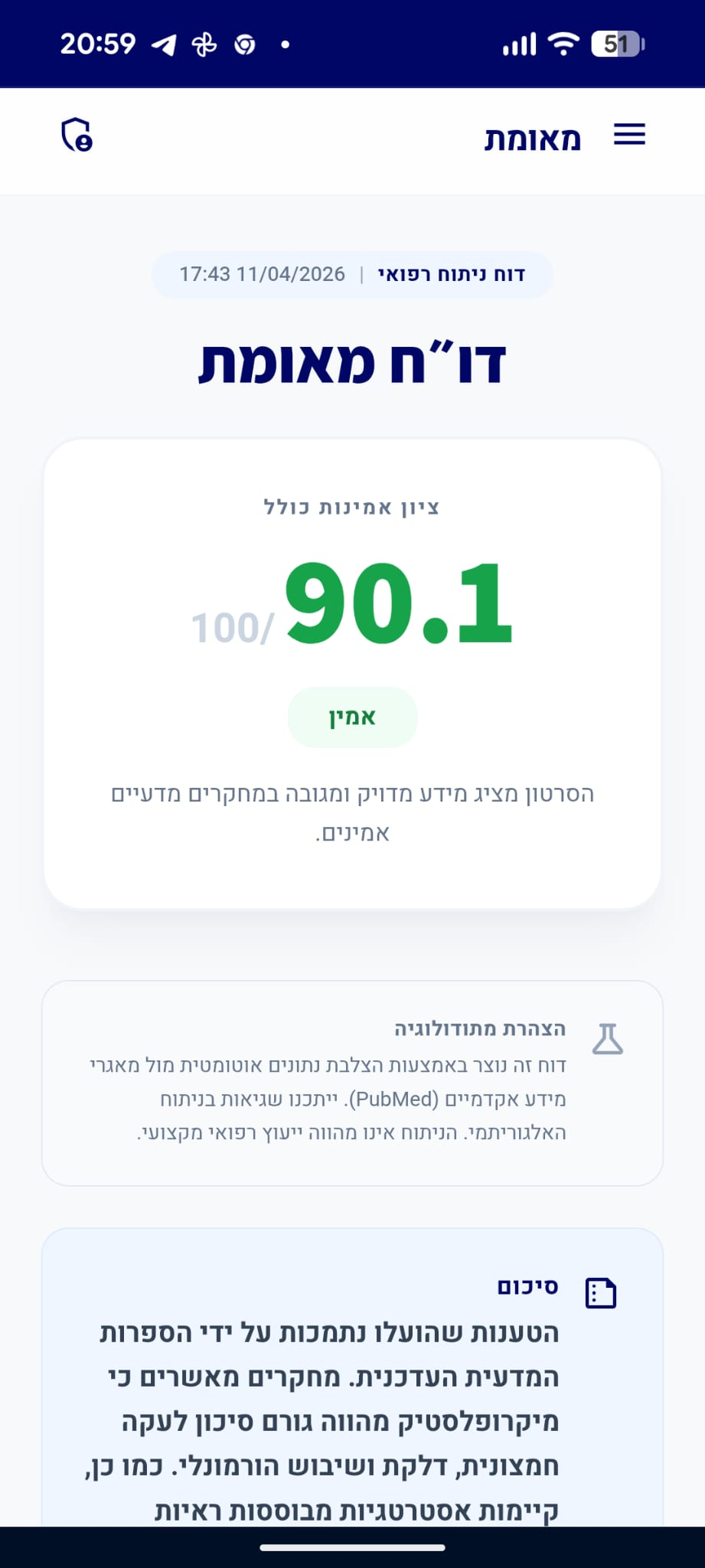
דו״ח מאומת
הסרטון מציג מידע מדויק ומגובה במחקרים מדעיים אמינים.
סיכום
הקליפ טען כי אין לקחת כדורים לשיכוך כאבים וכי כאב אוזניים נובע מחסימה רגשית, בעוד המומחה הדגיש כי ניהול כאב הוא קריטי להצלת חיים במצבים רפואיים דחופים כמו שברי צלעות או התקפי לב. הספרות המדעית תומכת בבירור בעמדת המומחה, ומאשרת כי כאב לא מטופל עלול להוביל לסיבוכים מסכני חיים, וכי קיימות אינטראקציות תרופתיות מורכבות שיש לקחת בחשבון. הטענות שהועלו בקליפ נגד שימוש בתרופות אינן מבוססות מדעית ומסכנות את המטופל.
דוח על סרטון תגובה
סרטון זה מציג קליפ של אדם המביע טענות רפואיות, ומומחה/מגיב שמתייחס אליהן. הציון מבוסס רק על טענות המומחה.
quiz טענות הקליפ ותגובת המומחה
"כאבי אוזניים נגרמים מחסימה או מחוסר יכולת לשמוע אחרים או את עצמך."
info המומחה לא התייחס ישירות לטענה זו ואין מספיק נתונים לבדיקה עצמאית
"אין לקחת משככי כאבים כי הם אינם בריאים ואינם מועילים."
"טיפול בכאב יכול להציל חיים, למשל בשברים בצלעות שבהם כאב לא מטופל פוגע בנשימה ומעלה סיכון לסיבוכים ריאתיים."
המומחה מסביר שמשככי כאבים הם חיוניים במצבים רפואיים מסוימים כדי למנוע סיבוכים מסכני חיים.
מסקנת הבדיקה:
הספרות הרפואית מאשרת כי כאב משמעותי משברים בצלעות מוביל להפחתת עומק הנשימה, מה שמעלה משמעותית את הסיכון לדלקת ריאות וכשל נשימתי. ניהול כאב אגרסיבי הוא חלק בלתי נפרד מהטיפול המקובל למניעת סיבוכים אלו. (🟩)
chevron_right מקורות מדעיים: (3)
-
link
Comprehensive Review of Current Pain Management in Rib Fractures With Practical Guidelines for Clinicians.
Rib fractures are present in 15% of all traumas and 60% of patients with chest traumas. Rib fractures are not life-threatening in isolation, but they can be quite painful which leads to splinting and compromise of respiratory function. Splinting limits the ability of a patient to take a deep breath, which leads to atelectasis, atelectasis to poor secretion removal, and poor secretion removal leads to pneumonia. Pneumonia is the common pathway to respiratory failure in patients with rib fractures. It is noted that in the elderly, each rib fracture increases developing pneumonia by 27% and the risk of dying by 19%. From a public health perspective, rib fractures have long-term implications with only 59% of patients returning to work at 6 months. In this review we will examine the state of art as it currently exists with regard to the management of pain associated with rib fractures. Included in this overview will be a brief review of the anatomy of the thorax and some important physiologic concepts, the latest trends in pharmacologic and noninvasive means of managing rib pain, a special section on epidural anesthesia, some other alternative invasive methods of pain control, and a review of the recent literature on rib plating. Finally, a practical, easy to follow guideline, to manage the patient with pain from rib fractures will be presented.…
PMID: 36600614
-
link
New horizons in rib fracture management in the older adult.
Adults aged ≥60 years now represent the majority of patients presenting with major trauma. Falls are the most common cause of injury, accounting for nearly three-quarters of all traumas in this population. Trauma to the thorax represents the second most common site of injury in this population, and is often associated with other serious injuries. Mortality rates are 2-5 times higher in older adults compared to their younger counterparts, often despite equivalent injury severity scores. Risk scoring systems have been developed to identify rib fracture patients at high risk of deterioration. Overall mortality from rib fractures is high, at approximately 10% for all ages. Mortality and morbidity from rib fractures primarily derive from pain-induced hypoventilation, pneumonia and respiratory failure. The main goal of care is therefore to provide sufficient analgesia to allow respiratory rehabilitation and prevent pulmonary complications. The provision of analgesia has evolved to incorporate novel regional anaesthesia techniques into conventional multimodal analgesia. Analgesia algorithms may aid early aggressive management and escalation of pain control. The current role for surgical fixation of rib fractures remains unclear for older adults who have been underrepresented in the research literature. Older adults with rib fractures often have multi-morbidity and frailty which complicate their injuries. Trauma services are evolving, and increasingly geriatricians will be embedded into trauma services to deliver comprehensive geriatric assessment. This review aims to provide an evidence-based overview of the management of rib fractures for the physician treating older patients who have sustained trauma.…
PMID: 31858117
-
link
Non-surgical management and analgesia strategies for older adults with multiple rib fractures: A systematic review, meta-analysis, and joint practice management guideline from the Eastern Association for the Surgery of Trauma and the Chest Wall Injury Society.
Chest wall injury in older adults is a significant cause of morbidity and mortality. Optimal nonsurgical management strategies for these patients have not been fully defined regarding level of care, incentive spirometry (IS), noninvasive positive pressure ventilation (NIPPV), and the use of ketamine, epidural, and other locoregional approaches to analgesia. Relevant questions regarding older patients with significant chest wall injury with patient population(s), intervention(s), comparison(s), and appropriate selected outcomes were chosen. These focused on intensive care unit (ICU) admission, IS, NIPPV, and analgesia including ketamine, epidural analgesia, and locoregional nerve blocks. A systematic literature search and review were conducted, our data were analyzed qualitatively and quantitatively, and the quality of evidence was assessed per the Grading of Recommendations Assessment, Development, and Evaluation methodology. No funding was used. Our literature review (PROSPERO 2020-CRD42020201241, MEDLINE, EMBASE, Cochrane, Web of Science, January 15, 2020) resulted in 151 studies. Intensive care unit admission was qualitatively not superior for any defined cohort other than by clinical assessment. Poor IS performance was associated with prolonged hospital length of stay, pulmonary complications, and unplanned ICU admission. Noninvasive positive pressure ventilation was associated with 85% reduction in odds of pneumonia ( p < 0.0001) and 81% reduction in odds of mortality ( p = 0.03) in suitable patients without risk of airway loss. Ketamine use demonstrated no significant reduction in pain score but a trend toward reduced opioid use. Epidural and other locoregional analgesia techniques did not affect pneumonia, length of mechanical ventilation, hospital length of stay, or mortality. We do not recommend for or against routine ICU admission. We recommend use of IS to inform ICU status and conditionally recommend use of NIPPV in patients without risk of airway loss. We offer no recommendation for or against ketamine, epidural, or other locoregional analgesia. Systematic Review/Meta-analysis; Level IV.…
PMID: 36730672
"במקרה של כאב איסכמי חריף בחזה (התקף לב), ניתן לשקול שימוש במורפיום להפחתת פעילות מערכת העצבים הסימפתטית."
המומחה מדגים מצב קליני שבו שימוש בתרופות לשיכוך כאב הוא הכרחי ומציל חיים.
מסקנת הבדיקה:
השימוש במורפיום באוטם שריר הלב נבחן היסטורית כדרך להפחתת כאב ופעילות סימפתטית, והמנגנון הפיזיולוגי של הפחתת הדרייב הסימפטי מוכר בספרות הרפואית כבעל השפעה על העומס הלבבי. (🟩)
"הפתרון לכאבים הוא רפואה הוליסטית ולא שימוש בתרופות."
info המומחה לא התייחס ישירות לטענה זו ואין מספיק נתונים לבדיקה עצמאית
person_check טענות נוספות של המומחה
טענות שהמומחה הביע שאינן קשורות ישירות לטענה ספציפית בקליפ
"מורפיום עלול לעכב את הפעילות של תרופות נוגדות טסיות מסוג מעכבי P2Y12 כמו טיקגרלור, פרסוגרל וקלופידוגרל."
מסקנת הבדיקה:
קיימות ראיות מוצקות לכך שמתן מורפיום מעכב את ספיגתם של מעכבי P2Y12 דרך הפה, מה שעלול להפחית את יעילותם הקלינית המיידית בטיפול באוטם שריר הלב. (🟩)
chevron_right מקורות מדעיים: (2)
-
link
Effect of morphine use on oral P2Y12 platelet inhibitors in acute myocardial infarction: Meta-analysis.
Morphine is the recommended analgesic in acute myocardial infarction (AMI). This recommendation has come under scrutiny because of possible slow uptake of oral antiplatelet agents. We performed a meta-analysis of all available studies in AMI patients treated with prasugrel or ticagrelor (P2Y12 inhibitors) that reported use of morphine prior to loading the antiplatelet agents to critically assess the safety of co-administration of morphine and the newer P2Y12 inhibitors. Several sources were searched from inception to December 2017 with inclusion of eight studies, largely observational. Mean difference (MD) was calculated for continuous variables, and standardized mean difference (SMD) for platelet function was assessed by the various platelet assays, 2 h after the loading dose of oral P2Y12 inhibitors. Higher platelet activity was noted among morphine group [SMD = 0.8, 95% confidence interval (CI) = 0.4-1.1, p < 0.01]. Morphine use caused higher odds of "high residual platelet reactivity" at 2 h (odds = 3.3, 95 %CI = 2.2-5.1, p < 0.01). Ticagrelor reached a lower plasma concentration in morphine group (MD = -481.8 ng/ml, 95% CI = -841.2 to -122.4 ng/ml, p < 0.01) with a higher vomiting rate (odds = 5.3, 95% CI = 2.5-11.1, p < 0.01). However, the composite of in-hospital mortality, stroke, and re-infarction was not significantly different between the groups (p = 0.83). Co-administration of morphine with P2Y12 inhibitors possibly decreases their efficacy in platelet inhibition. However, this did not translate into higher adverse outcomes because of low event rates, inadequate for analysis. A large randomized study is needed to evaluate the narcotic-P2Y12 interaction.…
PMID: 31280824
-
link
The role of cangrelor in acute and high-risk PCI settings.
Dual antiplatelet therapy with acetylsalicylic acid (ASA) and an oral P2Y12 inhibitor is the standard of care to prevent thrombotic complications in patients with acute coronary syndromes undergoing percutaneous coronary intervention (PCI). However, the oral administration of P2Y12 inhibitors bears significant limitations in acute and high-risk PCIs, particularly in ST-elevation myocardial infarction (STEMI) patients, especially those presenting with cardiogenic shock (CS) and cardiac arrest (CA). In these cases, factors such as active vomiting, altered physiology, sedatives, mechanical ventilation, and therapeutic hypothermia can impair drug absorption, reducing the intended antiplatelet effect and increasing ischaemic risk. In these cases, intravenous antiplatelet strategies with ASA and cangrelor could guarantee adequate periprocedural platelet inhibition. Here, we discuss the role of cangrelor in acute and high-risk PCI settings. The pharmacokinetic and pharmacodynamic attributes of cangrelor are discussed first, underscoring the distinctive features that make cangrelor an attractive antiplatelet agent in acute PCI settings. The second part of the review summarizes the evidence from real-world studies that illustrate how cangrelor has been adopted in contemporary practice. Finally, we provide a practical guide to cangrelor use, including recommendations for transitioning from cangrelor to oral P2Y12 inhibitors after PCI.…
PMID: 40470562

Elay Cohen | לימודי רפואה בחו״ל
דירוג זה מבוסס על 9 דוחות אימות קודמים.

האם הדוח הזה היה מועיל לך?
מה היה פחות טוב? (רשות)
תודה על הפידבק!
עירעור על דוח זה
ספקו ראיות חדשות או הצביעו על אי דיוקים
נעדכן אותך על תוצאות הבדיקה
הוסיפו קישורים למחקרים או מקורות רפואיים מוכרים
העירעור נשלח בהצלחה!
המנוע המדעי שלנו יבדוק את הראיות שהגשתם. נעדכן אתכם באימייל עם התוצאות.
ניתוח מבוסס בינה מלאכותית
דוח זה נוצר באופן אוטומטי על ידי מערכת בינה מלאכותית ועשוי להכיל שגיאות, אי-דיוקים או מידע חלקי. הניתוח אינו מהווה ייעוץ רפואי, אבחנה או המלצה לטיפול, והוא אינו תחליף לדעתו של איש מקצוע רפואי מוסמך. יש להתייעץ עם רופא או מומחה מוסמך לפני קבלת כל החלטה רפואית. המידע מוצג לצרכי מידע כללי בלבד.
מידע זה מופק על ידי בינה מלאכותית ואינו מהווה תחליף לייעוץ רפואי מקצועי.