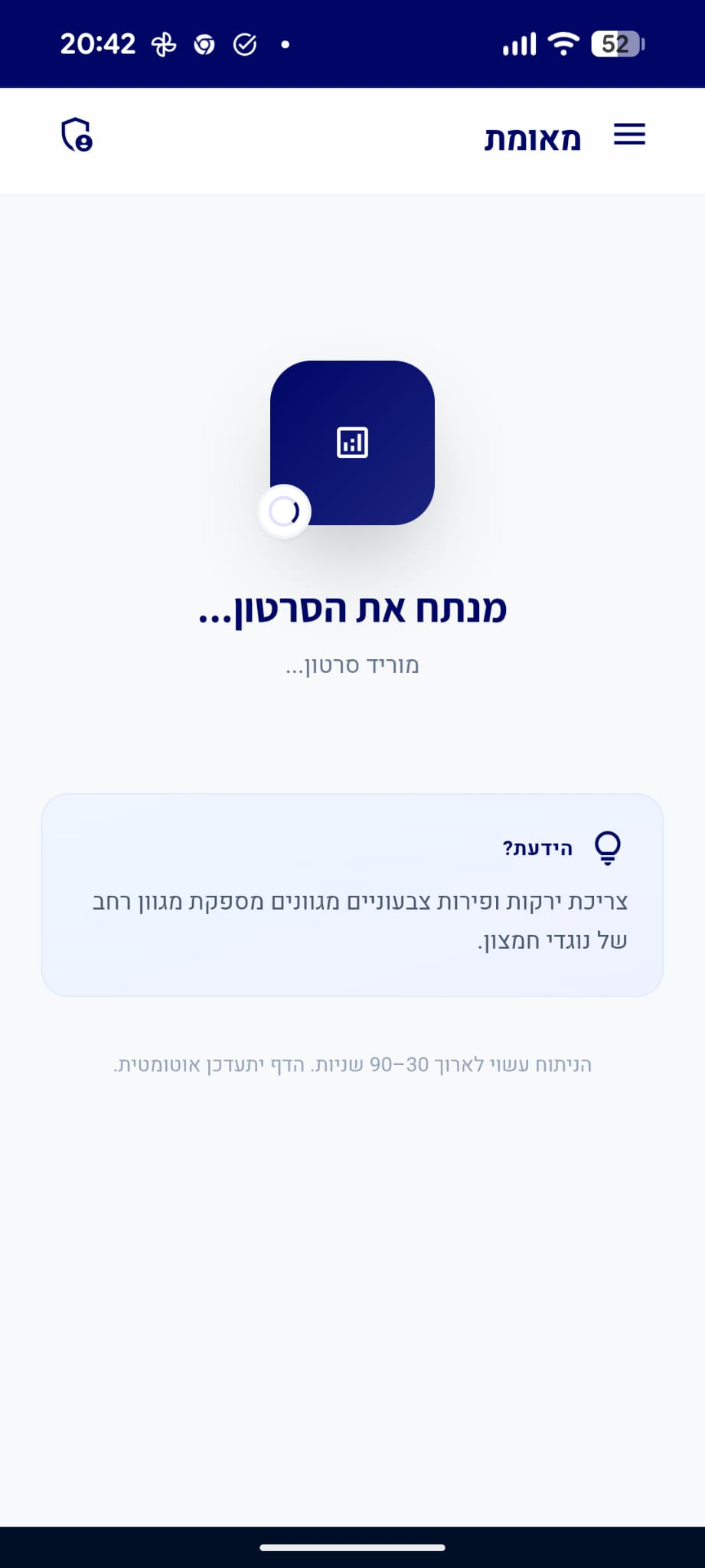
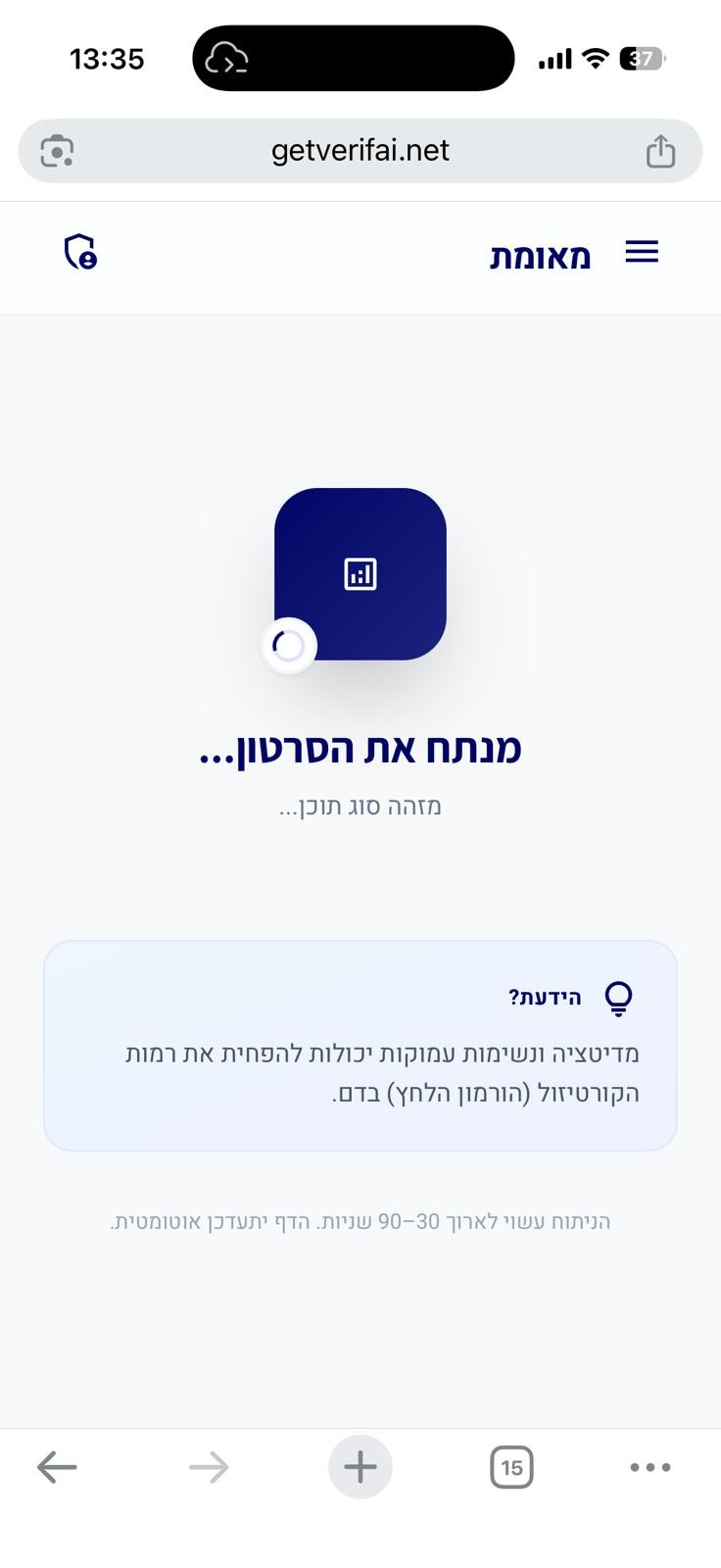
סריקה בתהליך...
הניתוח עשוי לארוך 30–90 שניות
הידעת?
הסרטון אינו מכיל תוכן רפואי
חושבים שחלה טעות?
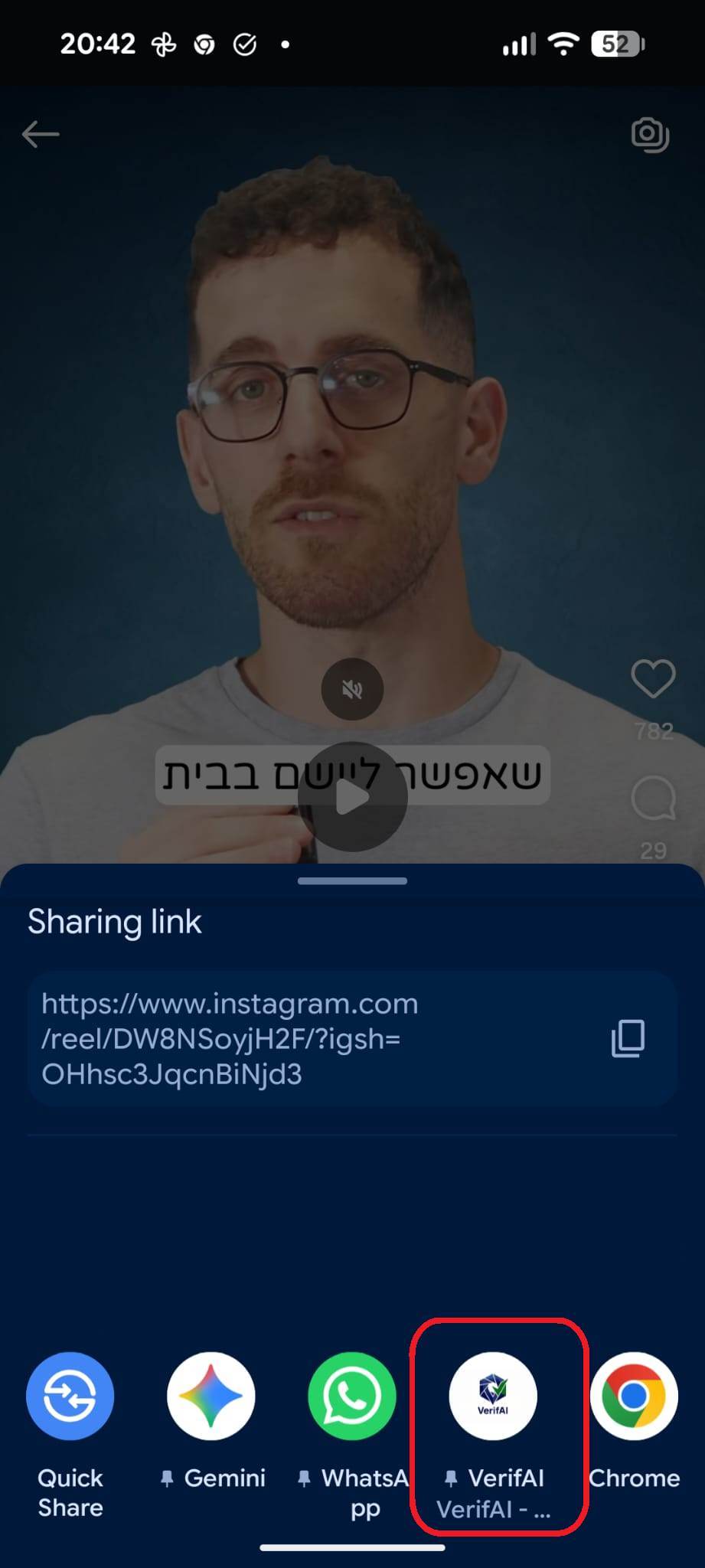
אם לדעתכם הסרטון אכן עוסק בטענות רפואיות או בריאותיות, הוסיפו הסבר קצר ושלחו בקשה לבדיקה מחדש.
הבקשה התקבלה! נבדוק את הסרטון ונחזור אליכם.
אירעה שגיאה בשליחת הבקשה. נסו שוב.
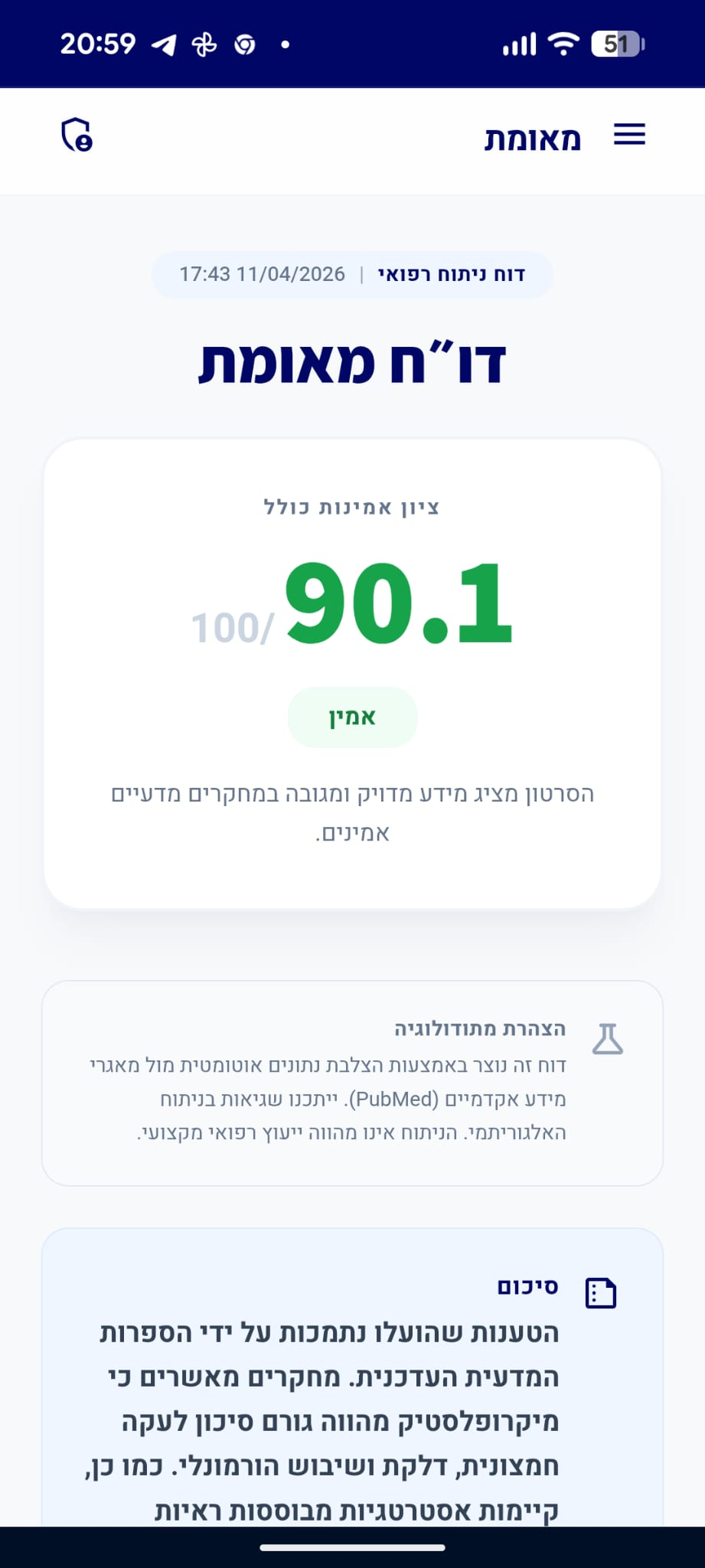
דו״ח מאומת
הסרטון מציג מידע מדויק ומגובה במחקרים מדעיים אמינים.
סיכום
כל הטענות שהוצגו לגבי צלוליט (השינוי המבני בעור) וצלוליטיס (הזיהום החיידקי) תואמות את הקונצנזוס המדעי וההנחיות הקליניות הקיימות ב-PubMed. קיימת הבחנה ברורה בספרות בין שני המצבים, והמידע שהוצג מדויק מבחינה רפואית.
analytics ניתוח טענות מבוסס ראיות
"צלוליט הוא שינוי מבני בעור שבו שומן תת-עורי בולט כלפי מעלה בעוד מחיצות רקמת חיבור מושכות את העור כלפי מטה."
מסקנת הבדיקה:
הספרות המדעית מאשרת כי צלוליט (Cellulite) הוא שינוי מבני ברקמות העור והתת-עור, המאופיין בבליטת שומן לתוך הדרמיס ובמשיכת העור כלפי מטה על ידי מחיצות רקמת חיבור (septae). (🟩)
chevron_right מקורות מדעיים: (3)
-
link
[Cellulite].
Cellulite is a condition affecting the dermal and subdermal compartment and developing on thighs and buttocks of almost every woman. Macroscopically, cellulite is characterized by dimpling, visible either spontaneously or after provoking maneuvers. While published concepts on the pathophysiology of cellulite are in parts inconclusive or contradictory, there are at least some recent studies describing or confirming structural and anatomic changes on dermal and subdermal tissues: (1) A gender specific dimorphism with subdermal septae oriented orthogonally towards the skin surface as well as protrusion of fat tissue into the dermis. (2) These intradermal fat protrusions additionally correlate with the presence of cellulite. (3) There is also a correlation between the thickness of the subdermal fat layer and the presence of cellulite. (4) Cellulite also correlates with focal hypertrophic subcutaneous septae and a reduced density of septae in general. Treatment of cellulite aims at (1) the reduction of the subcutaneous fat layer, (2) increase in dermal thickness and elasticity and (3) dissection of hypertrophic connective tissue septae, responsible for the most pronounced dermal indentions. A variety of treatment options have evolved ranging from topical retinol to interstitial laser.…
PMID: 20865236
-
link
Treatment of cellulite: Part I. Pathophysiology.
Cellulite is a topographic skin change that is nearly ubiquitous in postpubertal women. Treatment remains elusive. The various treatments currently available are only partially or temporarily effective. Newer therapeutic modalities continue to evolve without much understanding of the complex nature of cellulite. The successful treatment of cellulite will ultimately depend upon our understanding of the pathophysiology of cellulite adipose tissue. Part I of this two-part series on cellulite reviews how the concept and perception of cellulite has evolved over time and its proposed etiologies. The article also focuses on the physiology of human adipose tissue, particularly regarding cellulite.…
PMID: 20159304
-
link
Insights Into the Pathophysiology of Cellulite: A Review.
The etiology of cellulite is unclear. Treatment of cellulite has targeted adipose tissue, dermis, and fibrous septae with varying degrees of success and durability of response. Results from clinical trials that target different anatomical aspects of cellulite can provide insights into the underlying pathophysiology of cellulite. A search of the PubMed database and ClinicalTrials.gov website was conducted to identify clinical trials that have investigated treatments for cellulite. A lack of trial protocol standardization, objective means for quantification of improvement and reported cellulite severity, and short-term follow-up, as well as variation in assessment methods have made comparisons among efficacy studies challenging. However, the lack of durable efficacy and inconsistency seen in clinical results suggest that dermal or adipose tissue changes are not the primary etiologies of cellulite. Clinical studies targeting the collagen-rich fibrous septae in cellulite dimples through mechanical, surgical, or enzymatic approaches suggest that targeting fibrous septae is the strategy most likely to provide durable improvement of skin topography and the appearance of cellulite. The etiology of cellulite has not been completely elucidated. However, there is compelling clinical evidence that fibrous septae play a central role in the pathophysiology of cellulite.…
PMID: 32976174
"צלוליטיס הוא זיהום חיידקי של העור והרקמות שמתחתיו."
מסקנת הבדיקה:
צלוליטיס (Cellulitis) מוגדר בספרות הרפואית כזיהום חיידקי של העור והרקמות הרכות התת-עוריות, הנגרם לרוב על ידי חיידקים גראם-חיוביים. (🟩)
chevron_right מקורות מדעיים: (3)
-
link
Cellulitis.
Cellulitis is a common infection of the skin and subcutaneous tissue caused predominantly by gram-positive organisms. Risk factors include prior episodes of cellulitis, cutaneous lesions, tinea pedis, and chronic edema. Cellulitis is a clinical diagnosis and presents with localized skin erythema, edema, warmth, and tenderness. Uncomplicated cellulitis can be managed in the outpatient setting with oral antibiotics. Imaging often is not required but can be helpful. Recurrent cellulitis is common and predisposing conditions should be assessed for and treated at the time of initial diagnosis. For patients with frequent recurrences despite management of underlying conditions, antimicrobial prophylaxis can be effective.…
PMID: 33494874
-
link
Cellulitis: A Review of Pathogenesis, Diagnosis, and Management.
Cellulitis is a common skin infection resulting in increasing hospitalizations and health care costs. There is no gold standard diagnostic test, making cellulitis a potentially challenging condition to distinguish from other mimickers. Physical examination typically demonstrates poorly demarcated unilateral erythema with warmth and tenderness. Thorough history and clinical examination can narrow the differential diagnosis of cellulitis and minimize unnecessary hospitalization. Antibiotic selection is determined by patient history and risk factors, severity of clinical presentation, and the most likely microbial culprit.…
PMID: 34059247
-
link
Cellulitis: current insights into pathophysiology and clinical management.
Cellulitis is a bacterial skin and soft tissue infection which occurs when the physical skin barrier, the immune system and/or the circulatory system are impaired. Diabetes, obesity and old age are associated with defects in all of these areas and as a result are major predisposing factors for cellulitis. In this review, we summarise current insights into the pathophysiology of cellulitis and place the Dutch guidelines on the clinical management of cellulitis of the lower extremities in perspective. Recent evidence on diagnostic strategies is discussed, the importance of which is underscored by findings that venous insufficiency, eczema, deep vein thrombosis and gout are frequently mistaken for cellulitis. Empiric antibiotic choices are designed against the background of a low prevalence of multi-resistant Staphylococcus aureus. Novel antimicrobial agents registered for cellulitis are also discussed. Relapses occur frequently due to a high prevalence of risk factors associated with cellulitis in combination with the ccurrence of persistent post-inflammatory lymphatic damage. Lastly, we identify knowledge gaps which, if addressed, will advance our understanding of the pathophysiology of cellulitis and improve its clinical management.…
PMID: 29219814
"צלוליטיס מתפתח בדרך כלל כאשר חיידקים חודרים לעור דרך פתח כמו חתך, סדק או עקיצה."
מסקנת הבדיקה:
הספרות הרפואית מציינת כי צלוליטיס מתפתח לרוב כאשר שלמות העור נפגעת (כגון חתכים, עקיצות או סדקים), מה שמאפשר לחיידקים לחדור לרקמות העמוקות. (🟩)
chevron_right מקורות מדעיים: (2)
-
link
Cellulitis.
Cellulitis is a common infection of the skin and subcutaneous tissue caused predominantly by gram-positive organisms. Risk factors include prior episodes of cellulitis, cutaneous lesions, tinea pedis, and chronic edema. Cellulitis is a clinical diagnosis and presents with localized skin erythema, edema, warmth, and tenderness. Uncomplicated cellulitis can be managed in the outpatient setting with oral antibiotics. Imaging often is not required but can be helpful. Recurrent cellulitis is common and predisposing conditions should be assessed for and treated at the time of initial diagnosis. For patients with frequent recurrences despite management of underlying conditions, antimicrobial prophylaxis can be effective.…
PMID: 33494874
-
link
Cellulitis: current insights into pathophysiology and clinical management.
Cellulitis is a bacterial skin and soft tissue infection which occurs when the physical skin barrier, the immune system and/or the circulatory system are impaired. Diabetes, obesity and old age are associated with defects in all of these areas and as a result are major predisposing factors for cellulitis. In this review, we summarise current insights into the pathophysiology of cellulitis and place the Dutch guidelines on the clinical management of cellulitis of the lower extremities in perspective. Recent evidence on diagnostic strategies is discussed, the importance of which is underscored by findings that venous insufficiency, eczema, deep vein thrombosis and gout are frequently mistaken for cellulitis. Empiric antibiotic choices are designed against the background of a low prevalence of multi-resistant Staphylococcus aureus. Novel antimicrobial agents registered for cellulitis are also discussed. Relapses occur frequently due to a high prevalence of risk factors associated with cellulitis in combination with the ccurrence of persistent post-inflammatory lymphatic damage. Lastly, we identify knowledge gaps which, if addressed, will advance our understanding of the pathophysiology of cellulitis and improve its clinical management.…
PMID: 29219814
"תסמיני צלוליטיס כוללים אודם, נפיחות, חום מקומי וכאב."
מסקנת הבדיקה:
התסמינים הקליניים הקלאסיים של צלוליטיס כוללים אודם (erythema), נפיחות (edema), חום מקומי (warmth) וכאב או רגישות (tenderness). (🟩)
chevron_right מקורות מדעיים: (3)
-
link
Cellulitis: A Review of Pathogenesis, Diagnosis, and Management.
Cellulitis is a common skin infection resulting in increasing hospitalizations and health care costs. There is no gold standard diagnostic test, making cellulitis a potentially challenging condition to distinguish from other mimickers. Physical examination typically demonstrates poorly demarcated unilateral erythema with warmth and tenderness. Thorough history and clinical examination can narrow the differential diagnosis of cellulitis and minimize unnecessary hospitalization. Antibiotic selection is determined by patient history and risk factors, severity of clinical presentation, and the most likely microbial culprit.…
PMID: 34059247
-
link
Cellulitis: A Review.
Cellulitis is an infection of the deep dermis and subcutaneous tissue, presenting with expanding erythema, warmth, tenderness, and swelling. Cellulitis is a common global health burden, with more than 650,000 admissions per year in the United States alone. In the United States, an estimated 14.5 million cases annually of cellulitis account for $3.7 billion in ambulatory care costs alone. The majority of cases of cellulitis are nonculturable and therefore the causative bacteria are unknown. In the 15% of cellulitis cases in which organisms are identified, most are due to β-hemolytic Streptococcus and Staphylococcus aureus. There are no effective diagnostic modalities, and many clinical conditions appear similar. Treatment of primary and recurrent cellulitis should initially cover Streptococcus and methicillin-sensitive S. aureus, with expansion for methicillin-resistant S. aureus (MRSA) in cases of cellulitis associated with specific risk factors, such as athletes, children, men who have sex with men, prisoners, military recruits, residents of long-term care facilities, those with prior MRSA exposure, and intravenous drug users. Five days of treatment is sufficient with extension if symptoms are not improved. Addressing predisposing factors can minimize risk of recurrence. The diagnosis of cellulitis is based primarily on history and physical examination. Treatment of uncomplicated cellulitis should be directed against Streptococcus and methicillin-sensitive S. aureus. Failure to improve with appropriate first-line antibiotics should prompt consideration for resistant organisms, secondary conditions that mimic cellulitis, or underlying complicating conditions such as immunosuppression, chronic liver disease, or chronic kidney disease.…
PMID: 27434444
-
link
Cellulitis.
Cellulitis is a common infection of the skin and subcutaneous tissue caused predominantly by gram-positive organisms. Risk factors include prior episodes of cellulitis, cutaneous lesions, tinea pedis, and chronic edema. Cellulitis is a clinical diagnosis and presents with localized skin erythema, edema, warmth, and tenderness. Uncomplicated cellulitis can be managed in the outpatient setting with oral antibiotics. Imaging often is not required but can be helpful. Recurrent cellulitis is common and predisposing conditions should be assessed for and treated at the time of initial diagnosis. For patients with frequent recurrences despite management of underlying conditions, antimicrobial prophylaxis can be effective.…
PMID: 33494874
"צלוליטיס הוא מצב הדורש הערכה רפואית ולעיתים טיפול אנטיביוטי."
מסקנת הבדיקה:
צלוליטיס הוא מצב רפואי הדורש אבחנה קלינית על ידי איש מקצוע, והטיפול המקובל כולל מתן אנטיביוטיקה בהתאם לחומרת הזיהום. (🟩)
chevron_right מקורות מדעיים: (3)
-
link
Cellulitis.
Cellulitis is a common infection of the skin and subcutaneous tissue caused predominantly by gram-positive organisms. Risk factors include prior episodes of cellulitis, cutaneous lesions, tinea pedis, and chronic edema. Cellulitis is a clinical diagnosis and presents with localized skin erythema, edema, warmth, and tenderness. Uncomplicated cellulitis can be managed in the outpatient setting with oral antibiotics. Imaging often is not required but can be helpful. Recurrent cellulitis is common and predisposing conditions should be assessed for and treated at the time of initial diagnosis. For patients with frequent recurrences despite management of underlying conditions, antimicrobial prophylaxis can be effective.…
PMID: 33494874
-
link
Appropriate Use of Short-Course Antibiotics in Common Infections: Best Practice Advice From the American College of Physicians.
Antimicrobial overuse is a major health care issue that contributes to antibiotic resistance. Such overuse includes unnecessarily long durations of antibiotic therapy in patients with common bacterial infections, such as acute bronchitis with chronic obstructive pulmonary disease (COPD) exacerbation, community-acquired pneumonia (CAP), urinary tract infections (UTIs), and cellulitis. This article describes best practices for prescribing appropriate and short-duration antibiotic therapy for patients presenting with these infections. The authors conducted a narrative literature review of published clinical guidelines, systematic reviews, and individual studies that addressed bronchitis with COPD exacerbations, CAP, UTIs, and cellulitis. This article is based on the best available evidence but was not a formal systematic review. Guidance was prioritized to the highest available level of synthesized evidence.…
PMID: 33819054
-
link
Diagnosis and management of cellulitis.
Cellulitis is a frequently encountered condition, but remains a challenging clinical entity. Under and overtreatment with antimicrobials frequently occurs and mimics cloud the diagnosis. Typical presentation, microbiology and management approaches are discussed.…
PMID: 29626022

Elay Cohen | לימודי רפואה בחו״ל
דירוג זה מבוסס על 9 דוחות אימות קודמים.

האם הדוח הזה היה מועיל לך?
מה היה פחות טוב? (רשות)
תודה על הפידבק!
עירעור על דוח זה
ספקו ראיות חדשות או הצביעו על אי דיוקים
נעדכן אותך על תוצאות הבדיקה
הוסיפו קישורים למחקרים או מקורות רפואיים מוכרים
העירעור נשלח בהצלחה!
המנוע המדעי שלנו יבדוק את הראיות שהגשתם. נעדכן אתכם באימייל עם התוצאות.
ניתוח מבוסס בינה מלאכותית
דוח זה נוצר באופן אוטומטי על ידי מערכת בינה מלאכותית ועשוי להכיל שגיאות, אי-דיוקים או מידע חלקי. הניתוח אינו מהווה ייעוץ רפואי, אבחנה או המלצה לטיפול, והוא אינו תחליף לדעתו של איש מקצוע רפואי מוסמך. יש להתייעץ עם רופא או מומחה מוסמך לפני קבלת כל החלטה רפואית. המידע מוצג לצרכי מידע כללי בלבד.
מידע זה מופק על ידי בינה מלאכותית ואינו מהווה תחליף לייעוץ רפואי מקצועי.